5-month Academic project, Royal College of Art, 2025
5-month Academic project, Royal College of Art, 2025
5-month Academic project, Royal College of Art, 2025
STEP - TRANSFORMING UK SOCIAL PRESCRIBING FROM REACTIVE TREATMENT TO PROACTIVE PREVENTIVE HEALTHCARE
STEP - TRANSFORMING UK SOCIAL PRESCRIBING FROM REACTIVE TREATMENT TO PROACTIVE PREVENTIVE HEALTHCARE
STEP - TRANSFORMING UK SOCIAL PRESCRIBING FROM REACTIVE TREATMENT TO PROACTIVE PREVENTIVE HEALTHCARE
A systemic transformation plan aligning healthcare journeys with the NHS preventive care policy to resolve service awareness, operational staff overload, and data fragmentation.
A systemic transformation plan aligning healthcare journeys with the NHS preventive care policy to resolve service awareness, operational staff overload, and data fragmentation.
A systemic transformation plan aligning healthcare journeys with the NHS preventive care policy to resolve service awareness, operational staff overload, and data fragmentation.
Industry
Industry
Industry
Public Service - healthcare
Public Service - healthcare
Public Service - healthcare
My Role
My Role
My Role
Service Designer
Service Designer
Service Designer
Design With
Design With
Design With
London Brent Council;
Quay Health Solutions
London Brent Council; Quay Health Solutions
London Brent Council; Quay Health Solutions
Project Impacts
Project Impacts
Project Impacts
Award: Top 12
Award: Top 12
Award: Top 12
Selected for Helen Hamlyn Inclusive Design Awards, only 12 projects across all RCA MA programmes
Selected for Helen Hamlyn Inclusive Design Awards, only 12 projects across all RCA MA programmes
Selected for Helen Hamlyn Inclusive Design Awards, only 12 projects across all RCA MA programmes
UKRI-Funded Projects
UKRI-Funded Projects
UKRI-Funded Projects
Research insights fed into the discover&define process for the Green Social Prescribing initiative.
Research insights fed into the discover&define process for the Green Social Prescribing initiative.
Research insights fed into the discover&define process for the Green Social Prescribing initiative.
Expert Review
Expert Review
Expert Review
This project have identified those key constraints and challenges facing social prescribing and raised a critical ‘how might we...’ question with a clear vision in mind. This is exactly the social prescribing scheme needed ought it develop to its full potential.
This project have identified those key constraints and challenges facing social prescribing and raised a critical ‘how might we...’ question with a clear vision in mind. This is exactly the social prescribing scheme needed ought it develop to its full potential.
This project have identified those key constraints and challenges facing social prescribing and raised a critical ‘how might we...’ question with a clear vision in mind. This is exactly the social prescribing scheme needed ought it develop to its full potential.

Qian Sun
Green Social Prescribing Researcher
How Might We
How Might We
How Might We
how might we fully realise and maximise Link Workers’ unique value, leveraging the frontline nature of their role to create Social Prescribing as a proactive preventive care model?
Pilot leaders who are trying to innovate the service were trapped between accountability and evidence. Pulled in two directions, wanting to move, but without the roadmap or resources to show the way.
Pilot leaders who are trying to innovate the service were trapped between accountability and evidence. Pulled in two directions, wanting to move, but without the roadmap or resources to show the way.
The Overview
The Overview
The Overview
This case study is a service design research project developed at the Royal College of Art in partnership with Brent Council's Adult Healthcare team, while it situated at a pivotal moment for the NHS, as the 10-year plan repositions preventive and community-based care at the centre of the UK's health strategy.
Expert-endorsed, this project recognises that Social Prescribing is one of the key mechanisms through which that shift is meant to happen. But between policy ambition and operational reality, something was breaking down.
This case study is a service design research project developed at the Royal College of Art in partnership with Brent Council's Adult Healthcare team, while it situated at a pivotal moment for the NHS, as the 10-year plan repositions preventive and community-based care at the centre of the UK's health strategy.
Expert-endorsed, this project recognises that Social Prescribing is one of the key mechanisms through which that shift is meant to happen. But between policy ambition and operational reality, something was breaking down.
This case study is a service design research project developed at the Royal College of Art in partnership with Brent Council's Adult Healthcare team, while it situated at a pivotal moment for the NHS, as the 10-year plan repositions preventive and community-based care at the centre of the UK's health strategy.
Expert-endorsed, this project recognises that Social Prescribing is one of the key mechanisms through which that shift is meant to happen. But between policy ambition and operational reality, something was breaking down.
Project Highlights
Project Highlights
Project Highlights
This project sets out to find where and how to transform the service through:
co-designing with the staff within the public healthcare system who closest to the problem to build a shared picture of what needed to change, and why
working in alignment with GDS principles of user-centred, evidence-based public service design
moving the research between three scales: the lived experience of frontline workers, the organisational constraints shaping how the service was delivered, and the strategic levers available to shift it.
This project sets out to find where and how to transform the service through:
co-designing with the staff within the public healthcare system who closest to the problem to build a shared picture of what needed to change, and why
working in alignment with GDS principles of user-centred, evidence-based public service design
moving the research between three scales: the lived experience of frontline workers, the organisational constraints shaping how the service was delivered, and the strategic levers available to shift it.
Water-based communities face a mix of physical, social and financial challenges, from having to move their boats every two weeks to dealing with seasonal depression and isolation. But the deeper challenge was relational: many boaters had been the subject of research before, without seeing any improvement in their lives. That history made them defensive.
The discovery process therefore ran on two parallel tracks: one working with partner organisations using service design methods, one working directly with boaters using approaches drawn from sociological situationism under the pressure of limited trust.
Three Major Hierarchies, Three Needs,
In One System
Design Results
Design Results
Design Results
A comprehensive service transformation report including the research insights, process and design artefacts, giving decision-makers a strategic direction and frontline workers a practical framework and materials.
A strategic transition roadmap for Brent Council's Social Prescribing pilot
Grounded in Theory of Change and backcasting methods, the roadmap provided a phased pathway from the current reactive model toward proactive, community-led care.
A operational playbook for frontline workers
Based on the pilot's needs and physical resources, our team applied the participatory design workshops with frontline staff and pilot partners to create this toolkit set, including link worker's identity, how to initiate conversations and how to capture and reflect data.
A comprehensive service transformation report including the research insights, process and design artefacts, giving decision-makers a strategic direction and frontline workers a practical framework and materials.
A strategic transition roadmap for Brent Council's Social Prescribing pilot
Grounded in Theory of Change and backcasting methods, the roadmap provided a phased pathway from the current reactive model toward proactive, community-led care.
A operational playbook for frontline workers
Based on the pilot's needs and physical resources, our team applied the participatory design workshops with frontline staff and pilot partners to create this toolkit set, including link worker's identity, how to initiate conversations and how to capture and reflect data.
A comprehensive service transformation report including the research insights, process and design artefacts, giving decision-makers a strategic direction and frontline workers a practical framework and materials.
A strategic transition roadmap for Brent Council's Social Prescribing pilot
Grounded in Theory of Change and backcasting methods, the roadmap provided a phased pathway from the current reactive model toward proactive, community-led care.
A operational playbook for frontline workers
Based on the pilot's needs and physical resources, our team applied the participatory design workshops with frontline staff and pilot partners to create this toolkit set, including link worker's identity, how to initiate conversations and how to capture and reflect data.
We know how to support people early, but we don’t have the space or tools to do it properly.

Asma
Asma, Brent Council Link Worker
We know how to support people early, but we don’t have the space or tools to do it properly.
Asma
Asma, Brent Council Link Worker
I don’t know why it’s so hard to get people to come directly to us and just have a conversation.

Sen
QHS Link Worker
I don’t know why it’s so hard to get people to come directly to us and just have a conversation.
Sen
QHS Link Worker
Of course we want to make a difference; I can see what they (Link Workers) need, but how can I help them under limited time and resources?

Ketan Sheth
Brent Council SP pilot Leader
Of course we want to make a difference; I can see what they (Link Workers) need, but how can I help them under limited time and resources?
Ketan Sheth
Brent Council SP pilot Leader

20+
20+
20+
participants
participants
participants
7
7
7
deep interviews
deep interviews
deep interviews
5
5
5
cross-departmental workshops
cross-departmental workshops
cross-departmental workshops
1
1
1
Awards won
Awards won
Awards won
What did i create?
What did i create?
DESIGN DELIVER
DESIGN DELIVER
DESIGN DELIVER

Design 01
A strategic transition roadmap
Design 01
A strategic transition roadmap
The framework, at its core, repositions Social Prescribing from reactive to proactive, and this roadmap is built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces.
By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities.
By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.
The framework, at its core, repositions Social Prescribing from reactive to proactive, and this roadmap is built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces.
By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities.
By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.
The framework, at its core, repositions Social Prescribing from reactive to proactive, and this roadmap is built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces.
By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities.
By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.


Design Method - Transition Design
Design Method
Moving from reactive to proactive requires change at both levels simultaneously(the macro challenge of an outdated structure, and the micro challenge of disempowered Link Workers).
That's why together with team, we worked with Transition Design methods. Theory of Change mapped the conditions needed for systemic shift. Backcasting let us start from a preferred future and work backwards to identify the specific shifts in policy, funding, and practice needed to get there, horizon by horizon.
Moving from reactive to proactive requires change at both levels simultaneously(the macro challenge of an outdated structure, and the micro challenge of disempowered Link Workers).
That's why together with team, we worked with Transition Design methods. Theory of Change mapped the conditions needed for systemic shift. Backcasting let us start from a preferred future and work backwards to identify the specific shifts in policy, funding, and practice needed to get there, horizon by horizon.
Design Process
(click pictures to see details)
The roadmap didn't come from a stroke of inspiration. It was built through a series of co-design workshops with frontline Link Workers, pilot team leaders, and policy-connected stakeholders, grounding every horizon in what people inside the system said was actually achievable.
Co-design workshops with frontline staff (link workers, GPs) within and out NHS system
Co-design workshops with frontline staff (link workers, GPs) within and out NHS system
Workshops designed using Future Design methods, such as ‘future personas’ and the ‘Future Wheel’

to understand the operational reality and find their career developing potentials
+
Participatory design with decision-makers from council, national orgs and The King's Fund

Making complex information visual for discussing, such as ‘storyboard’ and ‘Theory of Change’



to design specific artefacts for creating the conditions for institutional alignment
Design 02
A operational Playbook
Design 02
A operational Playbook
Currently, Link Workers rely heavily on traditional approaches, primarily measuring shifts in patients’ wellbeing after interventions, sending flyers to introduce themselves and community activities.
They mentioned that those activities are not good at building trust and providing creative engagement with the public, so that people can’t remember this service well.
Meanwhile, they can’t recognise that they are a Link Worker, since there are no visible signals and direct space to show their identity. Users usually misunderstand their role with medical staff.

overview
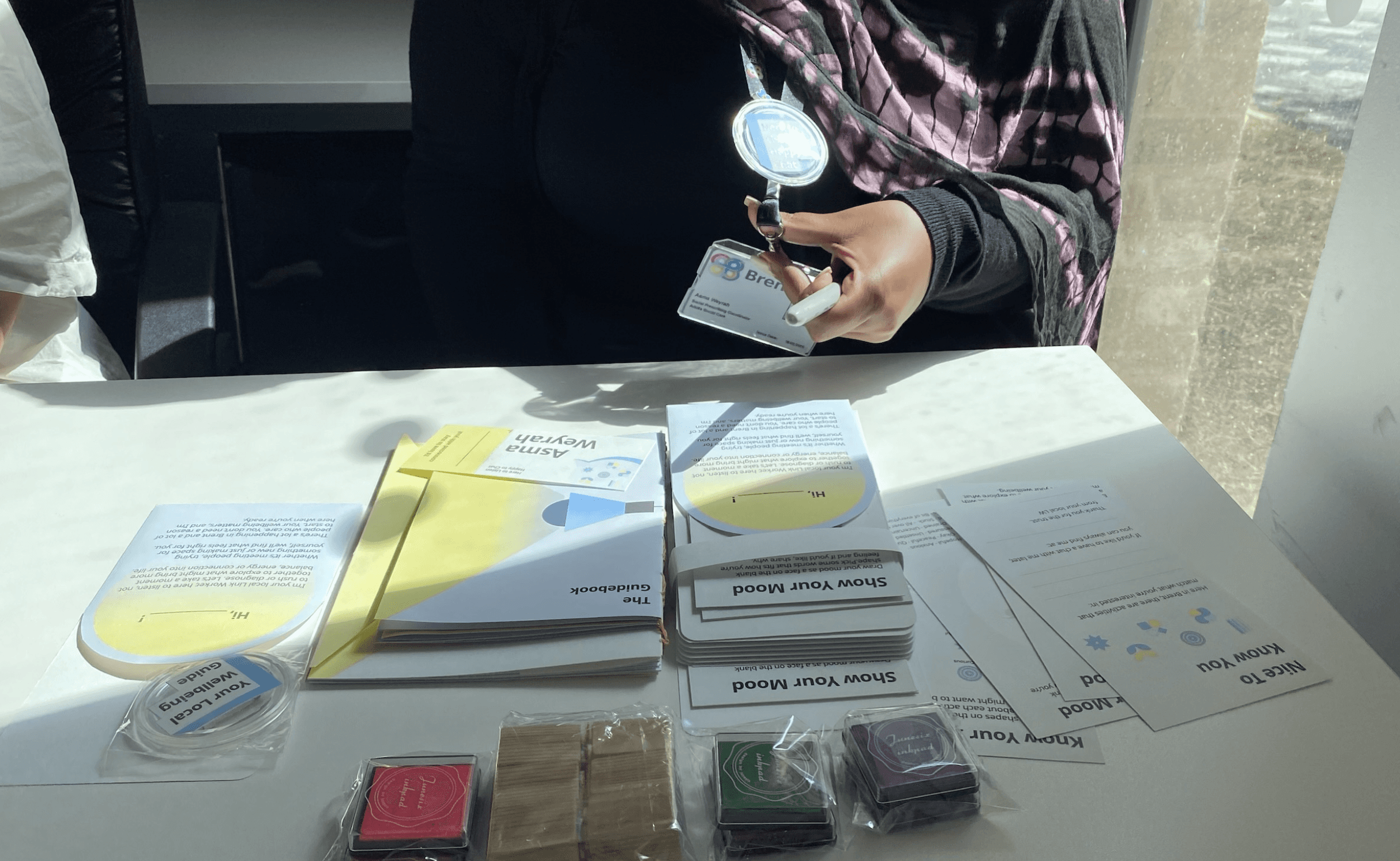
The toolkit includes several components, for internal and external use: a guidebook, notebook, badge, business card, toolkit cards, message pocket, follow-up email template and reflection questions.


overview
The toolkit includes several components, for internal and external use: a guidebook, notebook, badge, business card, toolkit cards, message pocket, follow-up email template and reflection questions.
The toolkit is designed for community-facing settings, helping Link Workers reach healthy individuals or those noticing health issues before a GP visit. It emphasises Link Workers as the central user in the service journey, starting with training and self-learning, followed by interactive community engagement, and ending with a peer reflection process to enhance professional identity and shared learning.

Design Process: Rapid Iteration

What did I build? What did I learn?
What did I build? What did I learn?
PROCESS & CHALLENGES
PROCESS & CHALLENGES
PROCESS & CHALLENGES
Three Major Hierarchies, Three Needs,
In One System
Three Major Hierarchies,
Three Needs,
In One System
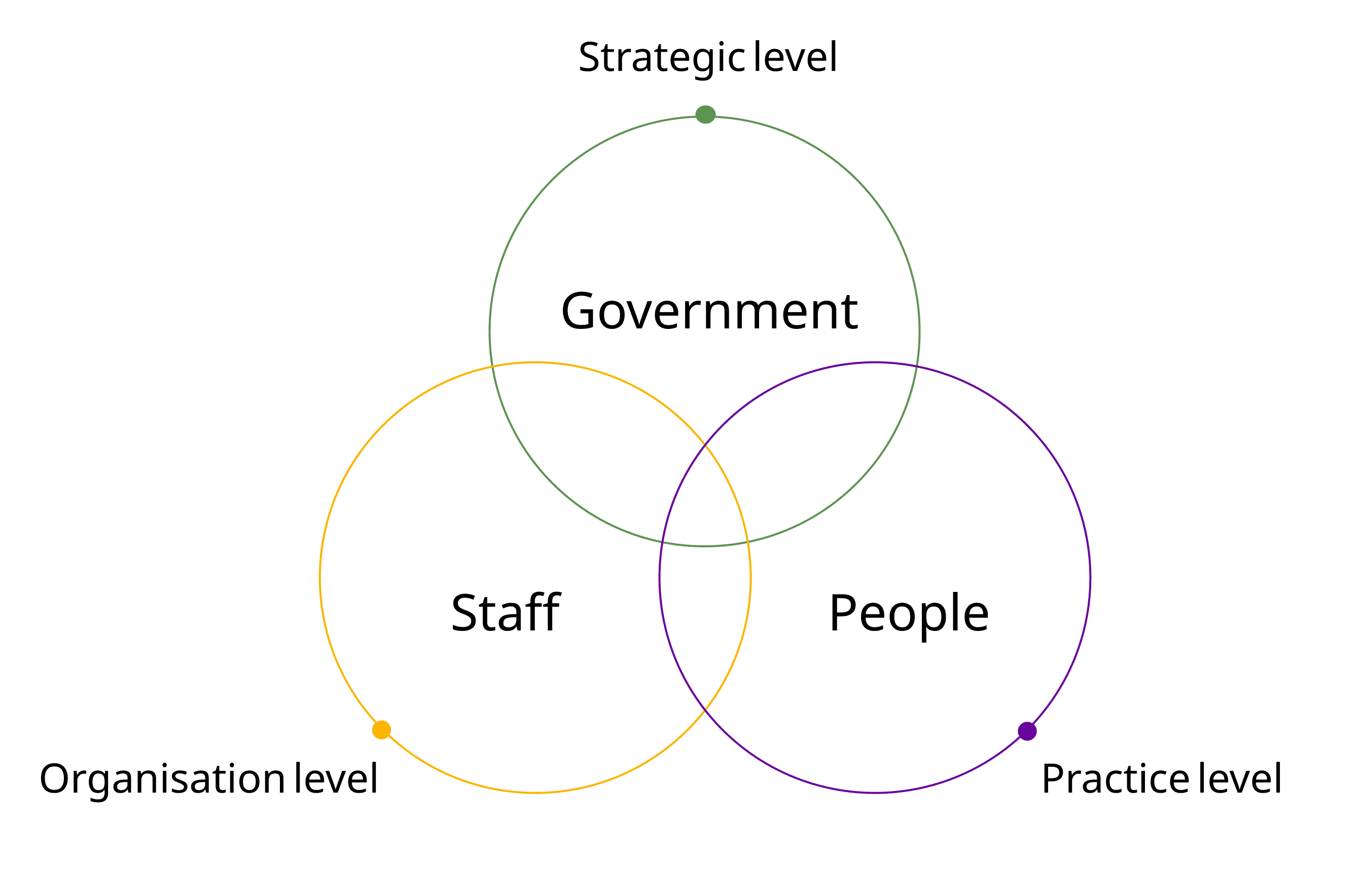
The research challenge was one of scale and translation. Each level of the system was describing a different crisis, and none of them were wrong. This made systems thinking not just a useful framework, but a necessary one. Only by understanding where these three sets of needs aligned, and where they conflicted, was it possible to identify the leverage points where design could intervene without displacing the problem elsewhere.
The research challenge was one of scale and translation. Each level of the system was describing a different crisis, and none of them were wrong. This made systems thinking not just a useful framework, but a necessary one. Only by understanding where these three sets of needs aligned, and where they conflicted, was it possible to identify the leverage points where design could intervene without displacing the problem elsewhere.

Social Prescribing is shaped at three different scales within one connected system: policy decisions at the top, organisational structures in the middle, frontline reality at the ground. Friction at any one level creates problems at the others.
Those invisable barriers are the real leverage points for solving problems
Those invisable barriers are the real leverage points for solving problems
The surface problems were visible: low service awareness, fragmented data capture, and frontline staff stretched beyond capacity.
However, they are not the core barrier. The deeper challenge was to identify that the core fiction was structural: a non-medical service built around reactive referral from medical staff that had never been redesigned to support long-term proactive preventative care.
The surface problems were visible: low service awareness, fragmented data capture, and frontline staff stretched beyond capacity.
However, they are not the core barrier. The deeper challenge was to identify that the core fiction was structural: a non-medical service built around reactive referral from medical staff that had never been redesigned to support long-term proactive preventative care.
Based on the data, currently 20% of GP appointments are non-medical.
Social Prescribing was built exactly for this, yet only 1.23% of those cases ever reach it.
Based on the data, currently 20% of GP appointments are non-medical.
Social Prescribing was built exactly for this, yet only 1.23% of those cases ever reach it.
Why are the figures so striking? Here is the questions I hold during this research journey:
Why are the figures so striking? Here is the questions I hold during this research journey:
On the ground, Link Workers are trained to help people early, so why can't they reach them?
why patients are unfamiliar with and distrustful of this service?
In the middle, organisations know their teams are struggling, so why aren't they stepping in?
At the top, policy is already committed to prevention, so why is the service still reactive?
On the ground, Link Workers are trained to help people early, so why can't they reach them?
why patients are unfamiliar with and distrustful of this service?
In the middle, organisations know their teams are struggling, so why aren't they stepping in?
At the top, policy is already committed to prevention, so why is the service still reactive?
Insight 1: Unrealised Link Worker's Values
Practice Level:
Unrealised Link Worker's Values
Insight 1: Unrealised Link Worker's Values
I spent time with Link Workers and other frontline staff directly, from shadowing, visiting community sites in Tower Hamlets and Brent Council, to interviewing frontline staff inside and outside the NHS. Then, I translated them into this current service blueprint for analysing the barriers and pain points.
I spent time with Link Workers and other frontline staff directly, from shadowing, visiting community sites in Tower Hamlets and Brent Council, to interviewing frontline staff inside and outside the NHS. Then, I translated them into this current service blueprint for analysing the barriers and pain points.

The pattern became clear. Link Workers never get the chance to be seen before they're needed.
Research data confirms what I was researching on the ground: after 3-4 years, many Link Workers report burnout, low job satisfaction and consider leaving (Oxford Link Worker Retention Study by Stephanie Tierney). High turnover doesn't just hurt individuals, it drains the system of the very relationships and local knowledge that took years to build.
Because they remain invisible to clients at the start of the journey, the essential foundation of trust is never built.
The pattern became clear. Link Workers never get the chance to be seen before they're needed.
Research data confirms what I was researching on the ground: after 3-4 years, many Link Workers report burnout, low job satisfaction and consider leaving (Oxford Link Worker Retention Study by Stephanie Tierney). High turnover doesn't just hurt individuals, it drains the system of the very relationships and local knowledge that took years to build.
Because they remain invisible to clients at the start of the journey, the essential foundation of trust is never built.
The pattern became clear. Link Workers never get the chance to be seen before they're needed.
Research data confirms what I was researching on the ground: after 3-4 years, many Link Workers report burnout, low job satisfaction and consider leaving (Oxford Link Worker Retention Study by Stephanie Tierney). High turnover doesn't just hurt individuals, it drains the system of the very relationships and local knowledge that took years to build.
Because they remain invisible to clients at the start of the journey, the essential foundation of trust is never built.
Insight 2: Limited Resources and Support Foction
Practice Level:
Unrealised Link Worker's Values
Insight 2: Limited Resources and Support Foction

After collecting pain point and needs from frontline workers, I brought them to the researchers, Brent pilot team leaders, and project managers connected to the service. I didn't find indifference. I found they were acutely aware of the problem and trying to figure out the clear problem statements and next step.
However, What emerged was a picture of a team caught in the middle.
Downward, they were responsible for keeping Link Workers supported and services running smoothly.
Upward, they needed to prove the value of Social Prescribing to policymakers to justify continued investment.
But without the data, metrics, and frameworks to demonstrate that innovation was sustainable, they couldn't make the case to the people above them.
After collecting pain point and needs from frontline workers, I brought them to the researchers, Brent pilot team leaders, and project managers connected to the service. I didn't find indifference. I found they were acutely aware of the problem and trying to figure out the clear problem statements and next step.
However, What emerged was a picture of a team caught in the middle.
Downward, they were responsible for keeping Link Workers supported and services running smoothly.
Upward, they needed to prove the value of Social Prescribing to policymakers to justify continued investment.
But without the data, metrics, and frameworks to demonstrate that innovation was sustainable, they couldn't make the case to the people above them.
After collecting pain point and needs from frontline workers, I brought them to the researchers, Brent pilot team leaders, and project managers connected to the service. I didn't find indifference. I found they were acutely aware of the problem and trying to figure out the clear problem statements and next step.
However, What emerged was a picture of a team caught in the middle.
Downward, they were responsible for keeping Link Workers supported and services running smoothly.
Upward, they needed to prove the value of Social Prescribing to policymakers to justify continued investment.
But without the data, metrics, and frameworks to demonstrate that innovation was sustainable, they couldn't make the case to the people above them.
Insight 3: Top-down? but now we need Bottom-up
Practice Level:
Unrealised Link Worker's Values
Insight 3: Top-down? but now we need Bottom-up
Through visualising Multi-Level Perspective (MLP) framework ↗︎ , which offers a holistic perspective on how change unfolds and helps identify the power shift, I could identify two key factors: how this service came into being, and why it has endured to this day:
Through visualising Multi-Level Perspective (MLP) framework ↗︎ , which offers a holistic perspective on how change unfolds and helps identify the power shift, I could identify two key factors: how this service came into being, and why it has endured to this day:

To be fair, this wasn't a design failure. When Social Prescribing was introduced in 2019, a structured referral pathway made sense. Public awareness of preventive care was low, people needed a channel to reach the service, and Link Workers as a role needed to be established within the system first. The model was right for its time.
But the time had moved, and the gap between policy intent and operational reality is widening. Moreover, transforming public services is a long game, especially policy in complex public systems is built top-down, which means structural change requires strategic decisions backed by compelling evidence.
To be fair, this wasn't a design failure. When Social Prescribing was introduced in 2019, a structured referral pathway made sense. Public awareness of preventive care was low, people needed a channel to reach the service, and Link Workers as a role needed to be established within the system first. The model was right for its time.
But the time had moved, and the gap between policy intent and operational reality is widening. Moreover, transforming public services is a long game, especially policy in complex public systems is built top-down, which means structural change requires strategic decisions backed by compelling evidence.
Research Perspective
My Aha Moment
(Research Insights)
My Aha Moment
(Research Insights)
My Aha Moment
(Research Insights)
Current medical system had created the invisibility and authority barriers for link worker to show their non-medical values
Link Workers are already everything the preventive healthcare system needed: the local knowledge, the trust, the human connection across multiple channels that no prescription can replicate.
System structure had blocked direct supports since without high-related data and cases to show the impact of service
Leaders working in the operational organisations who are trying to innovate the service are trapped between accountability and evidence. Pulled in two directions, wanting to move, but without the clear vision and resources to show the way.
Current system is not designed to meet the needs of future scenarios and policy developments
Policymakers have that power, but need compelling evidence to justify change for making long-term decisions.
Current medical system had created the invisibility and authority barriers for link worker to show their non-medical values
Link Workers are already everything the preventive healthcare system needed: the local knowledge, the trust, the human connection across multiple channels that no prescription can replicate.
System structure had blocked direct supports since without high-related data and cases to show the impact of service
Leaders working in the operational organisations who are trying to innovate the service are trapped between accountability and evidence. Pulled in two directions, wanting to move, but without the clear vision and resources to show the way.
Current system is not designed to meet the needs of future scenarios and policy developments
Policymakers have that power, but need compelling evidence to justify change for making long-term decisions.
Problem statement
Problem statement
Macro Level Outdated Structure
Macro Level Outdated Structure
The structural dependence on medical channels prevents Social Prescribing, a non-medical service, from reaching people early, limiting its potential as a genuinely preventive model of care.
The structural dependence on medical channels prevents Social Prescribing, a non-medical service, from reaching people early, limiting its potential as a genuinely preventive model of care.
Micro Level Disempowered Link Workers
Micro Level Disempowered Link Workers
Without role clarity, professional recognition, authority, and systemic support, Link Workers cannot act early and lead preventive care.
Without role clarity, professional recognition, authority, and systemic support, Link Workers cannot act early and lead preventive care.
What did I get?
What did I get?
EVALUATION
EVALUATION
EVALUATION
Design Highlights
Design Highlights
Design Highlights
The strategy landed where it mattered
Experts from The King's Fund described it as timely and aligned with national policy direction.
Brent Council's pilot team endorsed and adopted the definitions of "reactive" and "proactive", thought this strategy as a realistic, scalable step, a workable next move.
The toolkit changed how Link Workers showed up
For the first time, they reported feeling more visible, approachable, and confident to start conversations they couldn't start before.
The strategy landed where it mattered
Experts from The King's Fund described it as timely and aligned with national policy direction.
Brent Council's pilot team endorsed and adopted the definitions of "reactive" and "proactive", thought this strategy as a realistic, scalable step, a workable next move.
The toolkit changed how Link Workers showed up
For the first time, they reported feeling more visible, approachable, and confident to start conversations they couldn't start before.
The strategy landed where it mattered
Experts from The King's Fund described it as timely and aligned with national policy direction.
Brent Council's pilot team endorsed and adopted the definitions of "reactive" and "proactive", thought this strategy as a realistic, scalable step, a workable next move.
The toolkit changed how Link Workers showed up
For the first time, they reported feeling more visible, approachable, and confident to start conversations they couldn't start before.
What did I learn?
What did I learn?
Reflection
Reflection
Reflection
Public service innovation is an multidisciplinary endeavour.
Public service innovation is an multidisciplinary endeavour.
Public service innovation is an multidisciplinary endeavour.
"You can never understand a system by looking at any one part of it." — Russell Ackoff
"You can never understand a system by looking at any one part of it." — Russell Ackoff
I came into this project as a service designer. But the more I explored, the more I became a questioner: someone who looks for the unobvious, who maps what others overlook, who thinks alongside stakeholders rather than in front of them.
This project drew deliberately across service design, transition design, strategic design, and systems thinking, because each discipline offered something the others could not.
Public service innovation, I came to understand, It is a systemic problem that requires design, policy, organisational change, and community knowledge to be held in the same process, and for service designer, our key role is being willing to move between them without losing the thread.
I came into this project as a service designer. But the more I explored, the more I became a questioner: someone who looks for the unobvious, who maps what others overlook, who thinks alongside stakeholders rather than in front of them.
This project drew deliberately across service design, transition design, strategic design, and systems thinking, because each discipline offered something the others could not.
Public service innovation, I came to understand, It is a systemic problem that requires design, policy, organisational change, and community knowledge to be held in the same process, and for service designer, our key role is being willing to move between them without losing the thread.
Methodology 01
User-Centred Design
This project began with a commitment to understanding the people at the centre of service, not as a single user group. Link Workers, patients, GPs, and gov stakeholders each carry distinct needs, pressures, and degrees of power.
Methodology 02
Participatory Design
Co-design was woven into every stage of the project. Engaging stakeholders across the full spectrum of the ecosystem, such as pilot leaders, frontline staff, and political advocates, organisations such as The King's Fund, ensured that the design decisions were shaped by those who live and work within the system.
Methodology 03
Transition Design
Social Prescribing is a complex system, so Transition Design provided the framework to act on that complexity rather than just describe it. Tools, including Theory of Change and backcasting, allowed the project to give evidence-grounded direction for change.
Customers, users, citizens, staff, and what user-centred design actually means.
Customers, users, citizens, staff, and what user-centred design actually means.
Customers, users, citizens, staff, and what user-centred design actually means.
It also expanded how I define who I'm exploring for. In this project, the user was never just the public. Link Workers were equally at the centre. Exploring their reality was what made the difference between a solution that looked right on paper and one that could actually hold in practice. One of the most significant realisations was how I interpret the word “user-centred” in public service contexts. In service systems, there is no single user. There is a system of people, each of whom is both a user and a constraint on every other user's experience.
It also expanded how I define who I'm exploring for. In this project, the user was never just the public. Link Workers were equally at the centre. Exploring their reality was what made the difference between a solution that looked right on paper and one that could actually hold in practice. One of the most significant realisations was how I interpret the word “user-centred” in public service contexts. In service systems, there is no single user. There is a system of people, each of whom is both a user and a constraint on every other user's experience.
Special thanks to:
Special thanks to: