STEP
Social Prescribing Transition for Earlier Prevention
STEP
Social Prescribing Transition for Earlier Prevention
STEP reimagines the NHS preventive healthcare service in the UK, designing the transformation roadmap centred on the Social Prescribing to shift from reactive treatment to proactive prevention, innovating services into a more visible, inclusive and community-oriented model.

project Overview
What if the preventive care start with the human connection, not prescriptions?
What if the preventive care start with the human connection, not prescriptions?
What if the preventive care start with the human connection,
not prescriptions?
That's the premise behind Social Prescribing, a non-medical approach that treats loneliness, isolation, and inactivity not with medication, but by connecting people to community activities, green spaces, and peer support. STEP is a research-led service design project that I attempted to shrink the gap between what Social Prescribing promises and what's actually possible within the NHS. It aims to reposition Link Workers as proactive, public-facing agents of wellbeing by developing a long-term strategic vision and a practical toolkit service to embed it into a proactive prevention service in everyday life.
I partnered with Brent Council's Adult Healthcare Social Prescribing pilot team, also worked with a diverse group of staff, experts, policy makers (The King's Fund) and researchers (NASP), aligning on the same vision, learning from them who were trying to make this vision work, and co-designing solutions with them together that could actually work in practice.
The project was the chance to design for root causes, not just symptoms, so it was selected as one of the top 12 across all MA programmes at the RCA for the Helen Hamlyn Inclusive Design Awards, and its research has since fed into a UKRI-funded Green Social Prescribing initiative.
That's the premise behind Social Prescribing, a non-medical approach that treats loneliness, isolation, and inactivity not with medication, but by connecting people to community activities, green spaces, and peer support. STEP is a research-led service design project that I attempted to shrink the gap between what Social Prescribing promises and what's actually possible within the NHS. It aims to reposition Link Workers as proactive, public-facing agents of wellbeing by developing a long-term strategic vision and a practical toolkit service to embed it into a proactive prevention service in everyday life.
I partnered with Brent Council's Adult Healthcare Social Prescribing pilot team, also worked with a diverse group of staff, experts, policy makers (The King's Fund) and researchers (NASP), aligning on the same vision, learning from them who were trying to make this vision work, and co-designing solutions with them together that could actually work in practice.
The project was the chance to design for root causes, not just symptoms, so it was selected as one of the top 12 across all MA programmes at the RCA for the Helen Hamlyn Inclusive Design Awards, and its research has since fed into a UKRI-funded Green Social Prescribing initiative.
That's the premise behind Social Prescribing, a non-medical approach that treats loneliness, isolation, and inactivity not with medication, but by connecting people to community activities, green spaces, and peer support. STEP is a research-led service design project that I attempted to shrink the gap between what Social Prescribing promises and what's actually possible within the NHS. It aims to reposition Link Workers as proactive, public-facing agents of wellbeing by developing a long-term strategic vision and a practical toolkit service to embed it into a proactive prevention service in everyday life.
I partnered with Brent Council's Adult Healthcare Social Prescribing pilot team, also worked with a diverse group of staff, experts, policy makers (The King's Fund) and researchers (NASP), aligning on the same vision, learning from them who were trying to make this vision work, and co-designing solutions with them together that could actually work in practice.
The project was the chance to design for root causes, not just symptoms, so it was selected as one of the top 12 across all MA programmes at the RCA for the Helen Hamlyn Inclusive Design Awards, and its research has since fed into a UKRI-funded Green Social Prescribing initiative.
- Stakeholders engaged -
- Stakeholders engaged -






Role
Role
Service Designer
Service Designer
Duration
Duration
5 months, 2025
5 months, 2025
Industry
Industry
Public Sector
Public Sector
Design with
Design with
Royal College of Art
London Brent Council - Adult Healthcare Team
Royal College of Art
London Brent Council - Adult Healthcare Team
Related Topic
Related Topic
Public Service - Healthcare Transformation
Social Innovation
Public Service - Healthcare Transformation
Social Innovation
Methodology
User-Centred Design
This project began with a commitment to understanding the people at the centre of service, not as a single user group, but as individuals navigating very different positions within the same system.
Link Workers, patients, GPs, and gov stakeholders each carry distinct needs, pressures, and degrees of power. This shifted the project's lens from user satisfaction toward public health service equity.
This project began with a commitment to understanding the people at the centre of service, not as a single user group, but as individuals navigating very different positions within the same system.
Link Workers, patients, GPs, and gov stakeholders each carry distinct needs, pressures, and degrees of power. This shifted the project's lens from user satisfaction toward public health service equity.
Participatory Design
Co-design was not a method applied at the end, it was woven into every stage of the project. Engaging stakeholders across the full spectrum of the ecosystem, such as pilot leaders, frontline staff, and political advocates, organisations such as The King's Fund, ensured that the design decisions were shaped by those who live and work within the system.
Co-design was not a method applied at the end, it was woven into every stage of the project. Engaging stakeholders across the full spectrum of the ecosystem, such as pilot leaders, frontline staff, and political advocates, organisations such as The King's Fund, ensured that the design decisions were shaped by those who live and work within the system.
Transition Design
Social Prescribing is a complex system, exists at multiple scales, and is interconnected and interdependent. Transition Design provided the framework to act on that complexity rather than just describe it.
Tools including Theory of Change and backcasting allowed the project to work backwards from a desired future state, identifying the shifts in mindset, budget, policy, and practice needed to get there, giving evidence-grounded direction for change.
Social Prescribing is a complex system, exists at multiple scales, and is interconnected and interdependent. Transition Design provided the framework to act on that complexity rather than just describe it.
Tools including Theory of Change and backcasting allowed the project to work backwards from a desired future state, identifying the shifts in mindset, budget, policy, and practice needed to get there, giving evidence-grounded direction for change.
Discover Stage
Site Visits & Observations
Literature research
Surveys & Interviews
Systems Thinking Map
STEEP+V
Define Stage
Stakeholder Map & Power Dynamics Map
As-is User Journey Map
Service Blueprint
Theory of Change
Develop Stage
Multi-level perspective(MLP)framework
Backcasting
Co-design Workshops
Role-play Workshops
Deliver Stage
To-be Journey Map
User Flow
Usability Testing
Stress Test

20+
20+
participants
participants
7
7
deep interviews
deep interviews
5
5
cross-departmental workshops
cross-departmental workshops
cross-departmental workshops
1
1
Awards won
Awards won
Project Research
Project
Research
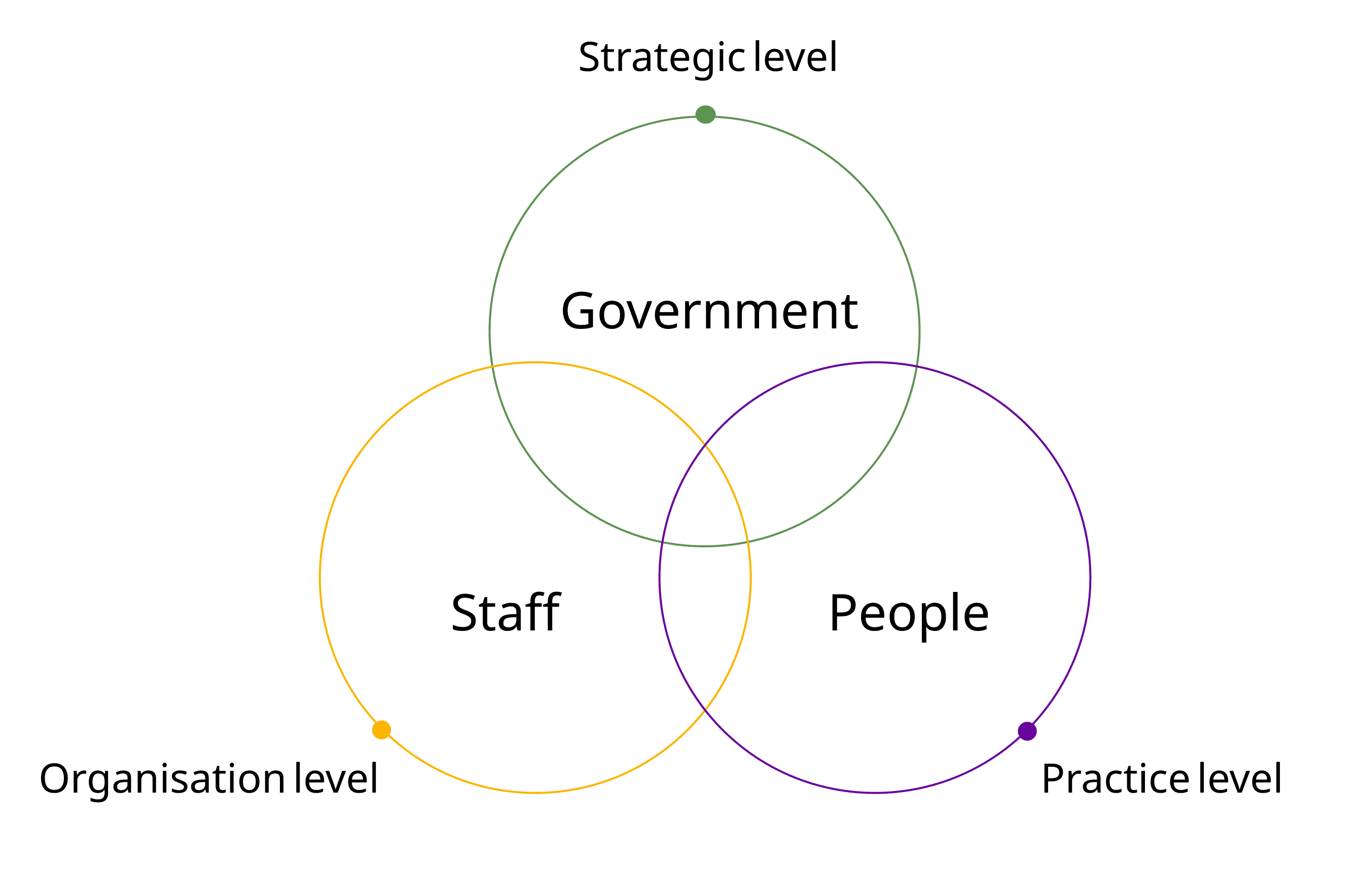
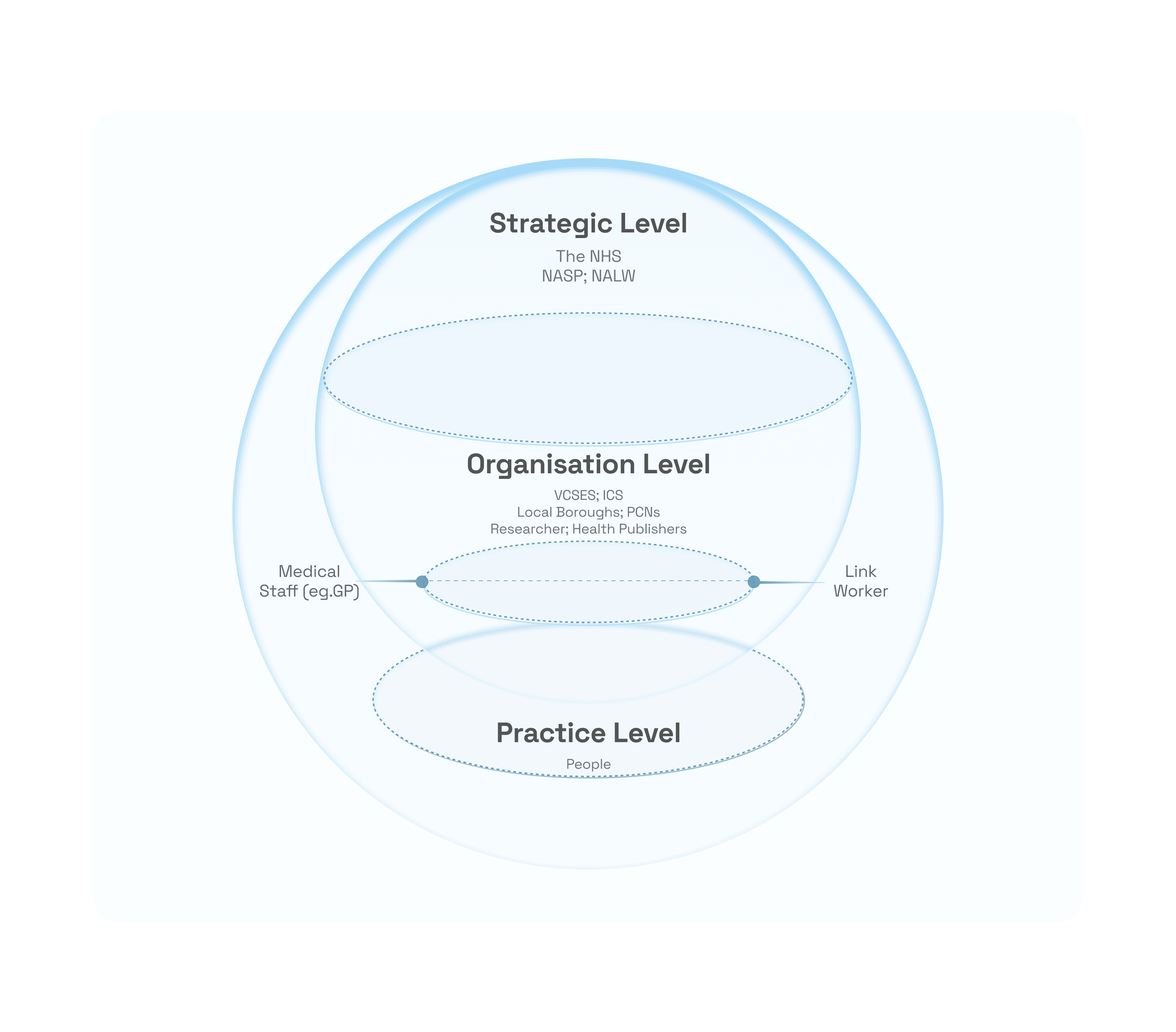
Three Major Hierarchies, Three Needs
Three Major Hierarchies, Three Needs
Early on, I realised Social Prescribing couldn't just innovate at one level, it's shaped by policy decisions at the top, filtered through organisational structures, and ultimately delivered by frontline in practice, such as Link Workers, GPs and community workers, who are navigating all of that in real time with public.
If I only looked at one layer, I'd miss how decisions at the top create friction at the bottom (or vice versa).
I needed to understand the system from all three angles, not just what Social Prescribing is supposed to be, but how it actually functions and where it breaks down. So I structured the research across Strategic, Organisational, and Practice levels, using different methods for each layer before connecting them within systemic view:
Early on, I realised Social Prescribing couldn't just innovate at one level, it's shaped by policy decisions at the top, filtered through organisational structures, and ultimately delivered by frontline in practice, such as Link Workers, GPs and community workers, who are navigating all of that in real time with public.
If I only looked at one layer, I'd miss how decisions at the top create friction at the bottom (or vice versa).
I needed to understand the system from all three angles, not just what Social Prescribing is supposed to be, but how it actually functions and where it breaks down. So I structured the research across Strategic, Organisational, and Practice levels, using different methods for each layer before connecting them within systemic view:
Early on, I realised Social Prescribing couldn't just innovate at one level, it's shaped by policy decisions at the top, filtered through organisational structures, and ultimately delivered by frontline in practice, such as Link Workers, GPs and community workers, who are navigating all of that in real time with public.
If I only looked at one layer, I'd miss how decisions at the top create friction at the bottom (or vice versa).
I needed to understand the system from all three angles, not just what Social Prescribing is supposed to be, but how it actually functions and where it breaks down. So I structured the research across Strategic, Organisational, and Practice levels, using different methods for each layer before connecting them within systemic view:

- Practice Level: Unrealised Values-
- Practice Level: Unrealised Values-
Methods: Literature research; Site Visits & Observations; Surveys & Interviews
Methods: Literature research; Site Visits & Observations; Surveys & Interviews
Methods: Literature research; Site Visits & Observations; Surveys & Interviews


After understanding how Social Prescribing actually operates day-to-day by completing 1 shadowing session with Link Worker, 3 community site visits across London (Tower Hamlets and Brent Council), and 4 interviews with frontline staff (Within/Outside the NHS organisation). Meanwhile, I reviewed the NHS policy documents and secondary research(i.e. University of Oxford studies led by Stephanie Tierney). When I mapped the as-is service blueprint to visualise the current operating model, it showed a clear gap: Link Workers have the potential to fully create their values, but structural barriers were limiting what they could actually deliver.
After understanding how Social Prescribing actually operates day-to-day by completing 1 shadowing session with Link Worker, 3 community site visits across London (Tower Hamlets and Brent Council), and 4 interviews with frontline staff (Within/Outside the NHS organisation). Meanwhile, I reviewed the NHS policy documents and secondary research(i.e. University of Oxford studies led by Stephanie Tierney). When I mapped the as-is service blueprint to visualise the current operating model, it showed a clear gap: Link Workers have the potential to fully create their values, but structural barriers were limiting what they could actually deliver.

We know how to support people early, but we don’t have the space or tools to do it properly.
Asma
Brent Council Link Worker
We know how to support people early, but we don’t have the space or tools to do it properly.
Asma
Brent Council Link Worker
I don’t know why it’s so hard to get people to come directly to us and just have a conversation.
Sen
QHS Link Worker
I don’t know why it’s so hard to get people to come directly to us and just have a conversation.
Sen
QHS Link Worker

- Organisational Level: Support Friction in System-
- Organisational Level: Support Friction in System-
Methods: Expert Interviews; Systems Thinking Mapping
Methods: Expert Interviews; Systems Thinking Mapping
Methods: Expert Interviews; Systems Thinking Mapping
While talking with Link Workers, they told me that, as an added role within the NHS system, they felt isolated, lacking peer support and overwhelmed by admin burden. Research data shows that after 3-4 years, many Link Workers report low job satisfaction and consider leaving. This raised a question: why wasn't the organisation providing support?
When I spoke with the team leaders from the Brent Council SP pilot team and QUAY HEALTH SOLUTIONS, I found they were acutely aware of the problem. As middle-layer actors in the system, they face pressure from two directions:
Downward accountability: They're responsible for keeping Link Workers supported and services running smoothly
Upward accountability: They need to prove values to policymakers to justify continued (or increased) systemic support
While talking with Link Workers, they told me that, as an added role within the NHS system, they felt isolated, lacking peer support and overwhelmed by admin burden. Research data shows that after 3-4 years, many Link Workers report low job satisfaction and consider leaving. This raised a question: why wasn't the organisation providing support?
When I spoke with the team leaders from the Brent Council SP pilot team and QUAY HEALTH SOLUTIONS, I found they were acutely aware of the problem. As middle-layer actors in the system, they face pressure from two directions:
Downward accountability: They're responsible for keeping Link Workers supported and services running smoothly
Upward accountability: They need to prove values to policymakers to justify continued (or increased) systemic support

The organisational level is trapped between wanting to innovate and lacking the strategic tools (data, metrics, frameworks) to demonstrate that the innovation is sustainable.
The organisational level is trapped between wanting to innovate and lacking the strategic tools (data, metrics, frameworks) to demonstrate that the innovation is sustainable.
Why use Systems Thinking Mapping for user research?
Why use Systems Thinking Mapping for user research?
Why use Systems Thinking Mapping for user research?
This service is a complex adaptive system, one where problems at different levels are not isolated but mutually reinforcing, both positive and negative. Systems thinking mapping allowed me to make these hidden connections visible, tracing feedback loops across policy, organisational, and practice levels simultaneously.
As Donella Meadows identified, the most powerful places to intervene in a system are not its most visible elements, but the underlying structures and feedback loops that govern its behaviour. In a system where top-down policy change moves slowly, this lens pointed us toward a different kind of leverage, one that could generate change from the bottom-up, and from within the existing structure.
This service is a complex adaptive system, one where problems at different levels are not isolated but mutually reinforcing, both positive and negative. Systems thinking mapping allowed me to make these hidden connections visible, tracing feedback loops across policy, organisational, and practice levels simultaneously.
As Donella Meadows identified, the most powerful places to intervene in a system are not its most visible elements, but the underlying structures and feedback loops that govern its behaviour. In a system where top-down policy change moves slowly, this lens pointed us toward a different kind of leverage, one that could generate change from the bottom-up, and from within the existing structure.
This service is a complex adaptive system, one where problems at different levels are not isolated but mutually reinforcing, both positive and negative. Systems thinking mapping allowed me to make these hidden connections visible, tracing feedback loops across policy, organisational, and practice levels simultaneously.
As Donella Meadows identified, the most powerful places to intervene in a system are not its most visible elements, but the underlying structures and feedback loops that govern its behaviour. In a system where top-down policy change moves slowly, this lens pointed us toward a different kind of leverage, one that could generate change from the bottom-up, and from within the existing structure.

- Strategic Level: Hierarchy barriers-
- Strategic Level: Hierarchy barriers-
Methods: MLP Framework; Power Dynamic Mapping
Methods: MLP Framework; Power Dynamic Mapping
Methods: MLP Framework; Power Dynamic Mapping
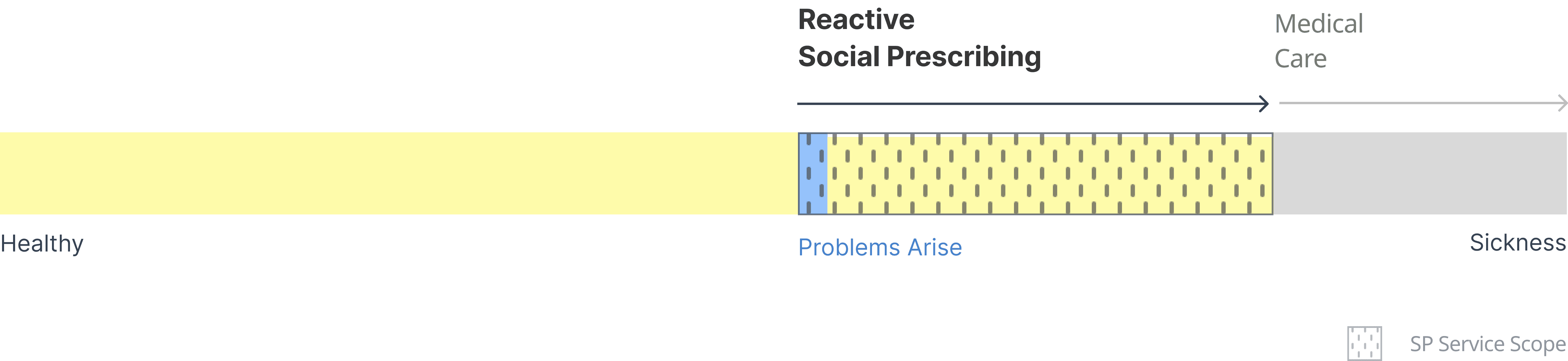

Since Social Prescribing was introduced to the NHS in 2019, the policy of healthcare priorities have fundamentally changed. The NHS's 10-year plan (2024) commits to three shifts: From hospital to community; From analogue to digital and From sickness to prevention. Social Prescribing sits at the heart of this new strategy. However, strategically, there's a deeper structural problem. Social Prescribing is trapped in a reactive model.
As the diagram shows, people only access it after they're sick enough to see their GP, meaning a non-medical service, designed for prevention, is gated by a medical bottleneck.
Since Social Prescribing was introduced to the NHS in 2019, the policy of healthcare priorities have fundamentally changed. The NHS's 10-year plan (2024) commits to three shifts: From hospital to community; From analogue to digital and From sickness to prevention. Social Prescribing sits at the heart of this new strategy. However, strategically, there's a deeper structural problem. Social Prescribing is trapped in a reactive model.
As the diagram shows, people only access it after they're sick enough to see their GP, meaning a non-medical service, designed for prevention, is gated by a medical bottleneck.
By mapping the Multi-Level Perspective (MLP) framework, I understood that Social Prescribing was introduced top-down. Structural change at this level requires strategic decision-making backed by evidence. The gap between policy intent and operational reality is widening. Policymakers have that power, but need compelling evidence to justify change.
By mapping the Multi-Level Perspective (MLP) framework, I understood that Social Prescribing was introduced top-down. Structural change at this level requires strategic decision-making backed by evidence. The gap between policy intent and operational reality is widening. Policymakers have that power, but need compelling evidence to justify change.
problem statement
problem
statement
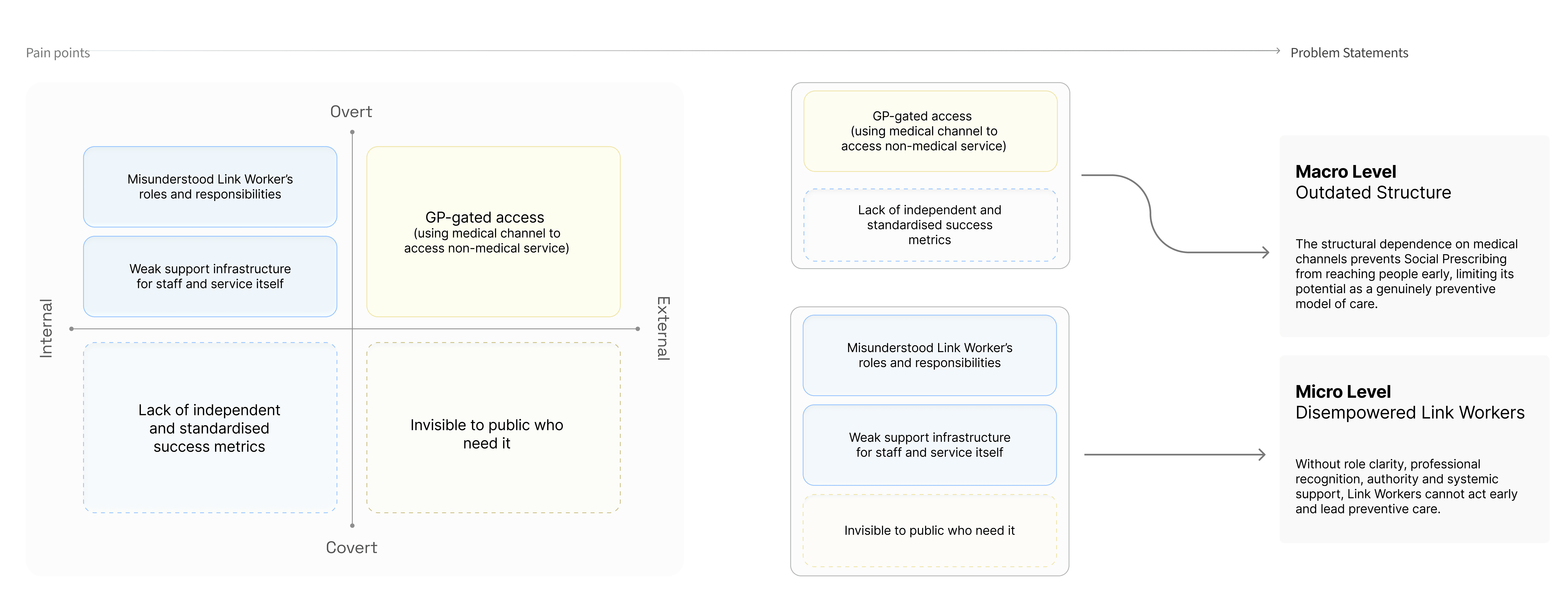
As I mapped these findings using systems thinking, a pattern became clear: these weren't isolated problems, they were interconnected barriers reinforcing each other across the system.
As I mapped these findings using systems thinking, a pattern became clear: these weren't isolated problems, they were interconnected barriers reinforcing each other across the system.
Macro Level – Outdated Structure
The structural dependence on medical channels prevents Social Prescribing from reaching people early, limiting its potential as a genuinely preventive model of care.
Macro Level – Outdated Structure
The structural dependence on medical channels prevents Social Prescribing from reaching people early, limiting its potential as a genuinely preventive model of care.
Micro Level – Disempowered Link Workers
Without role clarity, professional recognition, authority, and systemic support, Link Workers cannot act early and lead preventive care.
Micro Level – Disempowered Link Workers
Without role clarity, professional recognition, authority, and systemic support, Link Workers cannot act early and lead preventive care.
How Might We
How Might We
fully realise and maximise Link Workers’ unique value, leveraging the frontline nature of their role* to create Social Prescribing as a proactive preventive care model?
fully realise and maximise Link Workers’ unique value, leveraging the frontline nature of their role* to create Social Prescribing as a mature preventive care model?
fully realise and maximise Link Workers’ unique value, leveraging the frontline nature of their role to create Social Prescribing as a mature preventive care model?

Why Bottom-up?
Why Bottom-up?
Why Bottom-up?
Transforming public services from the top down is a long game, especially in complex systems like Social Prescribing; meaningful change often begins not at the policy level, but through the people already embedded within it.
The MLP framework offers a holistic perspective on how change unfolds and helps identify the power shift and where ground-level innovation could generate sufficient momentum to influence the regime from within.
Transforming public services from the top down is a long game, especially in complex systems like Social Prescribing; meaningful change often begins not at the policy level, but through the people already embedded within it.
The MLP framework offers a holistic perspective on how change unfolds and helps identify the power shift and where ground-level innovation could generate sufficient momentum to influence the regime from within.
Transforming public services from the top down is a long game, especially in complex systems like Social Prescribing; meaningful change often begins not at the policy level, but through the people already embedded within it.
The MLP framework offers a holistic perspective on how change unfolds and helps identify the power shift and where ground-level innovation could generate sufficient momentum to influence the regime from within.

Why Link Worker?
Why Link Worker?
Why Link Worker?
By organising service flows and user journey map, I can readily observe that:
Link Workers are uniquely positioned to be that starting point, they could be the leverage point to make changes.
They are the only actors who move across every level of the service, bridging organisational structures, policy realities, and direct community relationships.
They carry relational human trust with their clients that no clinical professional can replicate (Because they spend at least 360 hours or more with each of their clients to understand their true needs)
The rich local knowledge is their weapon, they have generated their own live map, enabling them to accurately and quickly locate available community-based services.
By organising service flows and user journey map, I can readily observe that:
Link Workers are uniquely positioned to be that starting point, they could be the leverage point to make changes.
They are the only actors who move across every level of the service, bridging organisational structures, policy realities, and direct community relationships.
They carry relational human trust with their clients that no clinical professional can replicate (Because they spend at least 360 hours or more with each of their clients to understand their true needs)
The rich local knowledge is their weapon, they have generated their own live map, enabling them to accurately and quickly locate available community-based services.
By organising service flows and user journey map, I can readily observe that:
Link Workers are uniquely positioned to be that starting point, they could be the leverage point to make changes.
They are the only actors who move across every level of the service, bridging organisational structures, policy realities, and direct community relationships.
They carry relational human trust with their clients that no clinical professional can replicate (Because they spend at least 360 hours or more with each of their clients to understand their true needs)
The rich local knowledge is their weapon, they have generated their own live map, enabling them to accurately and quickly locate available community-based services.

outcomes
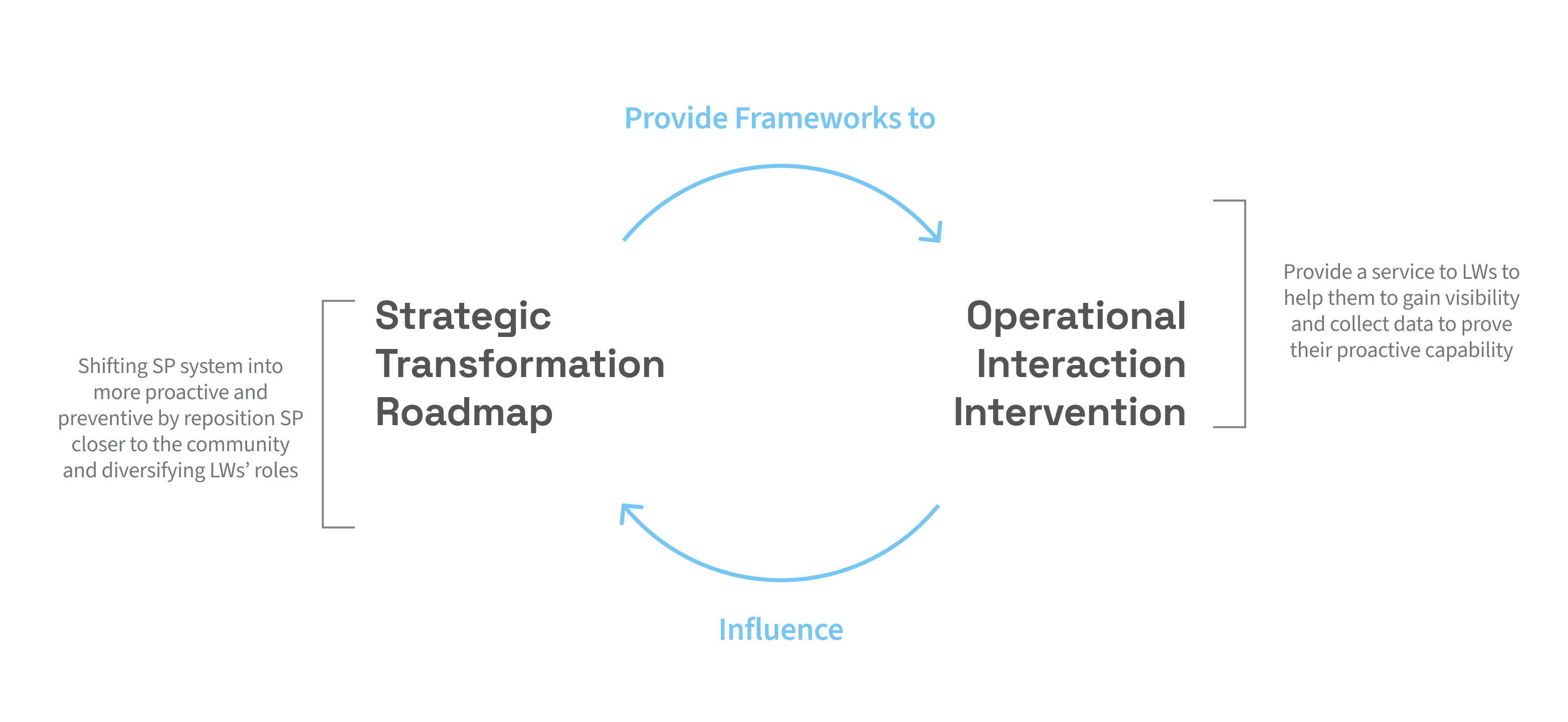
01 - Strategic Transformation Roadmap
01 - Strategic Transformation Roadmap
Today's model is largely reactive: it functions as a safety net, stepping in after a problem has already appeared to prevent things from getting worse. A proactive model works differently: it reaches people before problems take hold, supporting everyday wellbeing and building resilience rather than responding to a crisis.
This staged transformation roadmap built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces. By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities. By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.
Today's model is largely reactive: it functions as a safety net, stepping in after a problem has already appeared to prevent things from getting worse. A proactive model works differently: it reaches people before problems take hold, supporting everyday wellbeing and building resilience rather than responding to a crisis.
This staged transformation roadmap built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces. By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities. By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.
Today's model is largely reactive: it functions as a safety net, stepping in after a problem has already appeared to prevent things from getting worse. A proactive model works differently: it reaches people before problems take hold, supporting everyday wellbeing and building resilience rather than responding to a crisis.
This staged transformation roadmap built around the evolution of the Link Worker role across three horizons:
Beginning in 2025, Link Workers start moving beyond clinical settings, using practical tools to initiate proactive conversations in community spaces. By 2028, they become recognised, visible figures in local communities, trusted not just by patients but by communities. By 2040, Social Prescribing matures into Social Navigation: preventive care embedded into everyday life, delivered by a new generation of frontline professionals.

Theory of Change and Backcasting - Transition Design
Theory of Change and Backcasting - Transition Design
Moving from one to the other requires addressing both the macro challenge of an outdated system architecture and the micro challenge of disempowered frontline workers. That's why we decided to use transaction design methods in this project. Using the Theory of Change (above) to map the conditions needed for systemic shift, and using backcasting, we started from a preferred future and worked backwards to identify the shifts in policy, funding, and practice needed to get there.
Moving from one to the other requires addressing both the macro challenge of an outdated system architecture and the micro challenge of disempowered frontline workers. That's why we decided to use transaction design methods in this project. Using the Theory of Change (above) to map the conditions needed for systemic shift, and using backcasting, we started from a preferred future and worked backwards to identify the shifts in policy, funding, and practice needed to get there.

Co-design Workshops with stakeholders - Participatory Design
Co-design Workshops with stakeholders - Participatory Design
This roadmap did not emerge from a stroke of inspiration, but was developed through workshops co-designed with frontline staff and pilot team leaders, grounding the vision in the realities of those who live and work within the system every day.
Left: Co-design workshop with Link workers from both pilot and traditional medical settings to explore the role shift
Right: Imagine the future service scenario and challenges together with the pilot leader from Brent and NASP
This roadmap did not emerge from a stroke of inspiration, but was developed through workshops co-designed with frontline staff and pilot team leaders, grounding the vision in the realities of those who live and work within the system every day.
Left: Co-design workshop with Link workers from both pilot and traditional medical settings to explore the role shift
Right: Imagine the future service scenario and challenges together with the pilot leader from Brent and NASP
This roadmap did not emerge from a stroke of inspiration, but was developed through workshops co-designed with frontline staff and pilot team leaders, grounding the vision in the realities of those who live and work within the system every day.
Left: Co-design workshop with Link workers from both pilot and traditional medical settings to explore the role shift
Right: Imagine the future service scenario and challenges together with the pilot leader from Brent and NASP



02 - Operational Interaction Intervention
02 - Operational Interaction Intervention
Working closely with Brent Council's Social Prescribing pilot team, we got a chance to talk deeply with them, especially Link Workers in the team, to understand their current working barriers. Currently, Link Workers rely heavily on traditional approaches, primarily measuring shifts in patients’ wellbeing after interventions, sending flyers to introduce themselves and community activities. They mentioned about those activities is not good at building trust and providing creative engagement with public, so that people can’t remember this service well. Meanwhile, they can’t recognise they are Link Worker, since there is not visible signals to show their identity.
Working closely with Brent Council's Social Prescribing pilot team, we got a chance to talk deeply with them, especially Link Workers in the team, to understand their current working barriers. Currently, Link Workers rely heavily on traditional approaches, primarily measuring shifts in patients’ wellbeing after interventions, sending flyers to introduce themselves and community activities. They mentioned about those activities is not good at building trust and providing creative engagement with public, so that people can’t remember this service well. Meanwhile, they can’t recognise they are Link Worker, since there is not visible signals to show their identity.
Working closely with Brent Council's Social Prescribing pilot team, we got a chance to talk deeply with them, especially Link Workers in the team, to understand their current working barriers. Currently, Link Workers rely heavily on traditional approaches, primarily measuring shifts in patients’ wellbeing after interventions, sending flyers to introduce themselves and community activities. They mentioned about those activities is not good at building trust and providing creative engagement with public, so that people can’t remember this service well. Meanwhile, they can’t recognise they are Link Worker, since there is not visible signals to show their identity.
Co-Creation and Usability Test - Participatory Design
Co-Creation and Usability Test - Participatory Design
We presented three design directions and evaluated them together against real-world constraints(i.e. usability, cost, and implementation time) with the Brent Council team. After careful consideration, we have decided to proceed with the design direction of the toolkit.
Testing unfolded across three rounds.
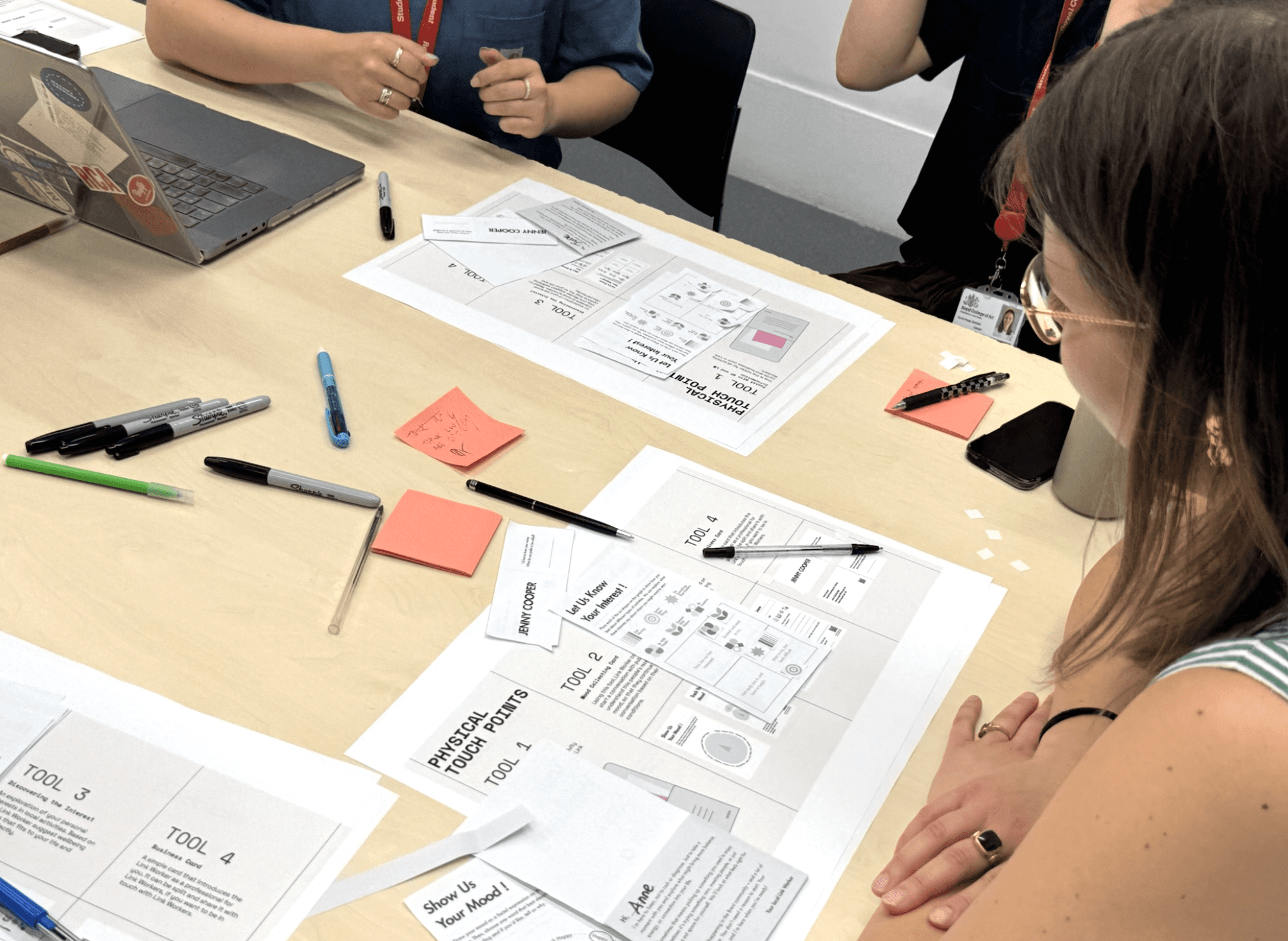
To refine the toolkit before introducing it to actual service users, we ran a series of role-play workshops. This approach was intentional: since our future vision involves engaging healthy members of the public rather than patients, we avoided testing immature ideas directly on vulnerable groups.
Each role-play involved over 8 participants of diverse ages and genders, simulating typical interactions Link Workers might have in community settings. Through these sessions, we explored public responses and validated the overall flow of conversations.
We presented three design directions and evaluated them together against real-world constraints(i.e. usability, cost, and implementation time) with the Brent Council team. After careful consideration, we have decided to proceed with the design direction of the toolkit.
Testing unfolded across three rounds.
To refine the toolkit before introducing it to actual service users, we ran a series of role-play workshops. This approach was intentional: since our future vision involves engaging healthy members of the public rather than patients, we avoided testing immature ideas directly on vulnerable groups.
Each role-play involved over 8 participants of diverse ages and genders, simulating typical interactions Link Workers might have in community settings. Through these sessions, we explored public responses and validated the overall flow of conversations.

The third round brought real Link Workers from Brent Council, sending the refined toolkit into the field to observe its impact in genuine community settings and capture feedback from the people and colleagues who would actually be using it day to day.
The third round brought real Link Workers from Brent Council, sending the refined toolkit into the field to observe its impact in genuine community settings and capture feedback from the people and colleagues who would actually be using it day to day.
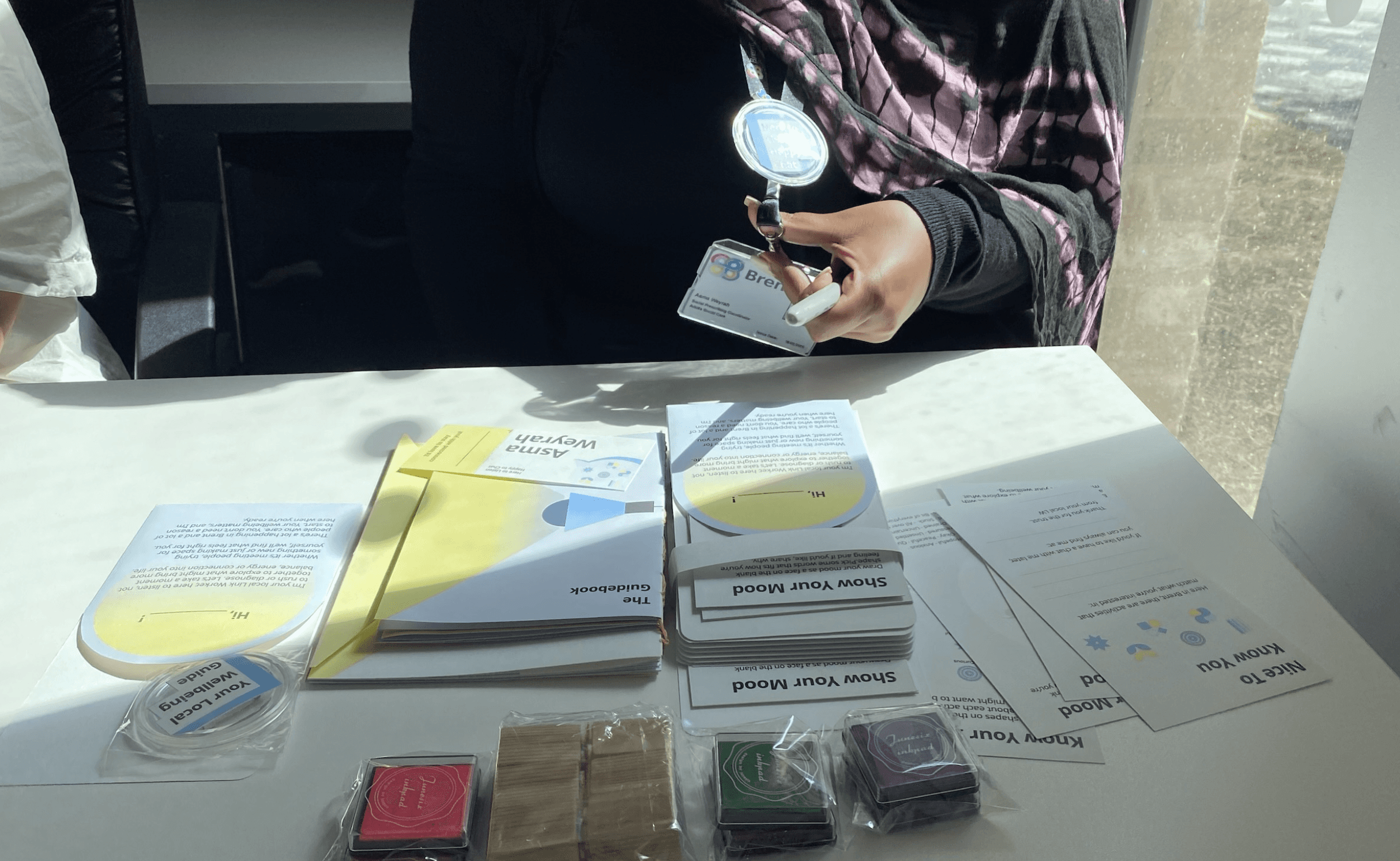
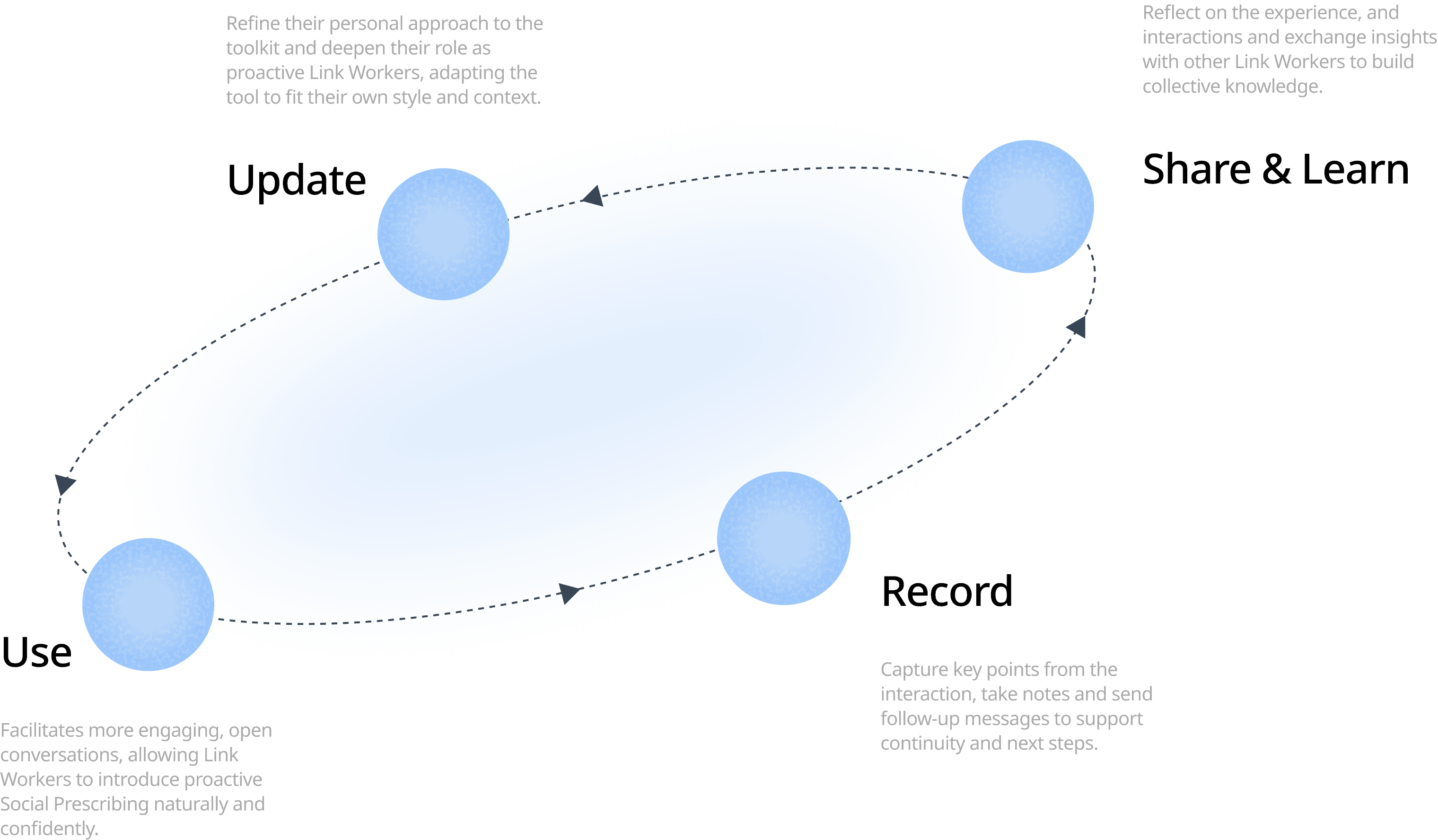
The toolkit is designed for community-facing settings(i.e. local events, public spaces, everyday encounters) where Link Workers can reach people who consider themselves healthy, or who are only beginning to notice something is off, long before a GP visit becomes necessary. At its core, the toolkit places Link Workers at the main user of the entire service journey:
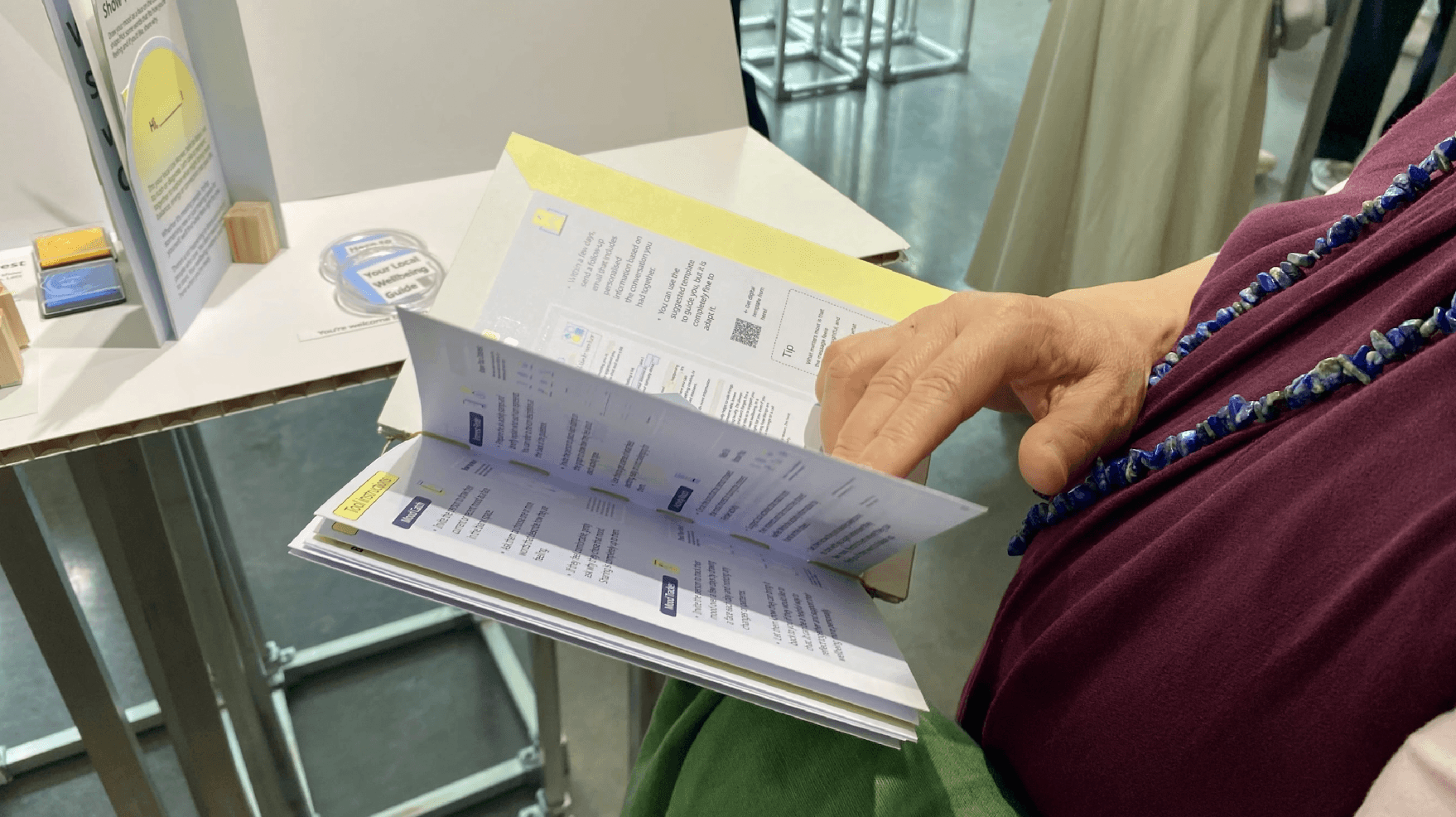
from an initial training guidebook that introduces the concept of proactive Social Prescribing and explains each component for self-learning, through to the live interaction with community residents with the role identity items(i.e. Business cards, badges, etc), and finally into a structured peer reflection process that strengthens professional identity and shared learning.
The toolkit is designed for community-facing settings(i.e. local events, public spaces, everyday encounters) where Link Workers can reach people who consider themselves healthy, or who are only beginning to notice something is off, long before a GP visit becomes necessary. At its core, the toolkit places Link Workers at the main user of the entire service journey:
from an initial training guidebook that introduces the concept of proactive Social Prescribing and explains each component for self-learning, through to the live interaction with community residents with the role identity items(i.e. Business cards, badges, etc), and finally into a structured peer reflection process that strengthens professional identity and shared learning.
The toolkit is designed for community-facing settings(i.e. local events, public spaces, everyday encounters) where Link Workers can reach people who consider themselves healthy, or who are only beginning to notice something is off, long before a GP visit becomes necessary. At its core, the toolkit places Link Workers at the main user of the entire service journey:
from an initial training guidebook that introduces the concept of proactive Social Prescribing and explains each component for self-learning, through to the live interaction with community residents with the role identity items(i.e. Business cards, badges, etc), and finally into a structured peer reflection process that strengthens professional identity and shared learning.

Highlight point:
The interaction itself is built around warmth and trust. It opens with a handwritten name exchange, a small gesture that proved consistently powerful across all testing rounds in dissolving the sense of boundary between professional and participant. For example, workshop testing validated the approach: 87% of participants described the experience as warm, welcoming, and human-centred, and 75% said it encouraged open, reflective conversation.
The interaction with public:
The conversation then moves through a mood drawing activity and an exploration of personal interests using icon stamps, inviting participants to discover what suits them through their own responses, rather than being prescribed a solution. This design choice was intentional: to convey a sense of self-empowerment, where people feel they are finding support, not being referred to it. The final step draws on something no system can replicate, the Link Worker's own knowledge of the local community. Each recommendation of a local activity is personalised, grounded in the unique relationships and contextual knowledge that Link Workers build over time. Afterwards, key insights are recorded in a notebook and followed up with a personalised email, building a trail of preventive impact that is rarely captured in traditional SP delivery.
Highlight point:
The interaction itself is built around warmth and trust. It opens with a handwritten name exchange, a small gesture that proved consistently powerful across all testing rounds in dissolving the sense of boundary between professional and participant. For example, workshop testing validated the approach: 87% of participants described the experience as warm, welcoming, and human-centred, and 75% said it encouraged open, reflective conversation.
The interaction with public:
The conversation then moves through a mood drawing activity and an exploration of personal interests using icon stamps, inviting participants to discover what suits them through their own responses, rather than being prescribed a solution. This design choice was intentional: to convey a sense of self-empowerment, where people feel they are finding support, not being referred to it. The final step draws on something no system can replicate, the Link Worker's own knowledge of the local community. Each recommendation of a local activity is personalised, grounded in the unique relationships and contextual knowledge that Link Workers build over time. Afterwards, key insights are recorded in a notebook and followed up with a personalised email, building a trail of preventive impact that is rarely captured in traditional SP delivery.
Highlight point:
The interaction itself is built around warmth and trust. It opens with a handwritten name exchange, a small gesture that proved consistently powerful across all testing rounds in dissolving the sense of boundary between professional and participant. For example, workshop testing validated the approach: 87% of participants described the experience as warm, welcoming, and human-centred, and 75% said it encouraged open, reflective conversation.
The interaction with public:
The conversation then moves through a mood drawing activity and an exploration of personal interests using icon stamps, inviting participants to discover what suits them through their own responses, rather than being prescribed a solution. This design choice was intentional: to convey a sense of self-empowerment, where people feel they are finding support, not being referred to it. The final step draws on something no system can replicate, the Link Worker's own knowledge of the local community. Each recommendation of a local activity is personalised, grounded in the unique relationships and contextual knowledge that Link Workers build over time. Afterwards, key insights are recorded in a notebook and followed up with a personalised email, building a trail of preventive impact that is rarely captured in traditional SP delivery.
solution's impact
How to measure the toolkit’s real-world impact?
How to measure the toolkit’s real-world impact?

Strategy Impact to Operational Level
Strategy Impact to Operational Level
Strategy Impact to Operational Level
Reflection
If there is one thing this project made clear, it is that service design is not a magic fix. It is a slow, often frustrating process of building trust, shifting ingrained mindsets, and carving out space for new ways of working.
Working in the public sector reshaped how I think about service design itself. Unlike designing a product/service, public service design operates on longer timelines, across more layers of stakeholders. Progress is rarely linear. Decisions made at a policy level take months to reach the frontline and by the time they do, the context has often shifted. Learning to work within that slowness, rather than against it, was one of the most important adjustments I made throughout this project.
It also changed how I think about users. In STEP, the "user" was never just the public. Link Workers, as the staff within system, were equally at the centre, navigating an under-resourced system, carrying relational labour that the system rarely acknowledged, and absorbing the consequences of every structural failure above them. Designing for both sides simultaneously, without flattening their very different needs into a single solution, was one of the hardest and most formative challenges of the project.
As Stickdorn and Schneider argues, “Service design thinking connects stakeholders to co-create value.” This experience also brought me face to face with the limits of design. A service designer cannot restructure a budget, pass a policy, or compel institutional change. What we can do is make the invisible visible, surface the needs of people whose voices rarely reach decision-makers, connect actors who operate in silos, and create the conditions for conversations that would not otherwise happen.
Real change in complex public systems demands collective, persistent effort over time. Designers can be catalysts, but the seeds we plant need the whole system to tend them.
If there is one thing this project made clear, it is that service design is not a magic fix. It is a slow, often frustrating process of building trust, shifting ingrained mindsets, and carving out space for new ways of working.
Working in the public sector reshaped how I think about service design itself. Unlike designing a product/service, public service design operates on longer timelines, across more layers of stakeholders. Progress is rarely linear. Decisions made at a policy level take months to reach the frontline and by the time they do, the context has often shifted. Learning to work within that slowness, rather than against it, was one of the most important adjustments I made throughout this project.
It also changed how I think about users. In STEP, the "user" was never just the public. Link Workers, as the staff within system, were equally at the centre, navigating an under-resourced system, carrying relational labour that the system rarely acknowledged, and absorbing the consequences of every structural failure above them. Designing for both sides simultaneously, without flattening their very different needs into a single solution, was one of the hardest and most formative challenges of the project.
As Stickdorn and Schneider argues, “Service design thinking connects stakeholders to co-create value.” This experience also brought me face to face with the limits of design. A service designer cannot restructure a budget, pass a policy, or compel institutional change. What we can do is make the invisible visible, surface the needs of people whose voices rarely reach decision-makers, connect actors who operate in silos, and create the conditions for conversations that would not otherwise happen.
Real change in complex public systems demands collective, persistent effort over time. Designers can be catalysts, but the seeds we plant need the whole system to tend them.
If there is one thing this project made clear, it is that service design is not a magic fix. It is a slow, often frustrating process of building trust, shifting ingrained mindsets, and carving out space for new ways of working.
Working in the public sector reshaped how I think about service design itself. Unlike designing a product/service, public service design operates on longer timelines, across more layers of stakeholders. Progress is rarely linear. Decisions made at a policy level take months to reach the frontline and by the time they do, the context has often shifted. Learning to work within that slowness, rather than against it, was one of the most important adjustments I made throughout this project.
It also changed how I think about users. In STEP, the "user" was never just the public. Link Workers, as the staff within system, were equally at the centre, navigating an under-resourced system, carrying relational labour that the system rarely acknowledged, and absorbing the consequences of every structural failure above them. Designing for both sides simultaneously, without flattening their very different needs into a single solution, was one of the hardest and most formative challenges of the project.
As Stickdorn and Schneider argues, “Service design thinking connects stakeholders to co-create value.” This experience also brought me face to face with the limits of design. A service designer cannot restructure a budget, pass a policy, or compel institutional change. What we can do is make the invisible visible, surface the needs of people whose voices rarely reach decision-makers, connect actors who operate in silos, and create the conditions for conversations that would not otherwise happen.
Real change in complex public systems demands collective, persistent effort over time. Designers can be catalysts, but the seeds we plant need the whole system to tend them.
- Thanks to -
- Thanks to -
Teammates: Liboyang Wang, Sooyoung Oh
Tutor group: John Makepeace and Professor Qian Sun
Teammates: Liboyang Wang, Sooyoung Oh
Tutor group: John Makepeace and Professor Qian Sun
Teammates: Liboyang Wang, Sooyoung Oh
Tutor group: John Makepeace and Professor Qian Sun

