Category
Service Design
Transition Design
Duration
Mar - Jun 2025
External collaborators

#Background
Social Prescribing (SP) is one of the UK’s most ambitious shifts toward preventive, community-based healthcare — aiming to connect people with non-clinical support. Since being formally integrated into NHS primary care in 2019, SP has gained increasing momentum, both nationally and globally. While still evolving, the UK is widely seen as a pioneer and global leader, over 30+ countries have started developing their own SP-inspired models, learning from the UK’s early investment and experimentation.
The World Health Organisation(WHO) has also endorsed SP as a promising pathway to tackle wider determinants of health, especially in addressing social isolation, inequality, and mental wellbeing.
At the centre of this system are Link Workers (LWs) — non-clinical professionals who get referrals from medical staff, support individuals holistically, build personalised plan with them and connect them to community-based services. Their work reflects the values of trust, relational care, and upstream support. But as the system grows, it faces new challenges: public awareness remains low, access is still tied to medical referrals, and many LWs operate in silos without systemic support.
I chose to focus on SP because it sits at the intersection of health equity, social wellbeing, and public service transformation where design can help shift systems, not just services. SP offers a rare chance to reimagine care around what people actually need.
SP is not a broken system, it’s still young and rapidly evolving. If left to grow without intentional design, it risks becoming a service that disappears in obscurity, failing to meet the diverse needs of communities or achieve its full potential. This moment presents a critical opportunity: to shape the direction of SP while it’s still flexible, and to embed values like accessibility, trust, and prevention before the system hardens.
From the outset, we approached SP as a complex social system involving actors at multiple levels — from NHS policy and local councils to frontline Primary Care Networks (PCNs), Link Workers and community organisations. To navigate this, we used Systems Thinking and Mapping (Figure3. System thinking map) to understand both macro and micro dynamics. We used this method to map both positive and negative feedback loops across the Social Prescribing system, revealing how GPs, Link Workers, patients, and councils interact. It exposed both enabling structures and systemic barriers.
One key insight was a recurring negative loop: lack of institutional support → LW burnout → high turnover → fragmented delivery → reduced impact → less investment → continued lack of support.
This mapping exercise helped us identify key leverage points for intervention, like particularly around visibility, role clarity, and community engagement.

#Research methodologies
To understand the service as it currently operates, we used a mix of desk and field research methods:
>Desk research: Reviewing NHS documents, University of Oxford studies lead by Stephanie Tierney, The National Academy for Social Prescribing (NASP) reports, and the public articles from The King’s Fund, etc.
>Interviews and site visits: Conducting in-depth conversations with Link Workers, service managers, and policy researchers; visiting SP sites in Tower Hamlets, the Bromley by Bow Centre and Brent Council in London.
>Service Blueprinting: Synthesising ten months of SP delivery into a single service flow, revealing that LWs are the key relational node connecting people across clinical and non-clinical support. (Figure2. Service blueprint)
We distilled the unique value of Link Workers across short- and long-term horizons:
Reducing GP workload
Improving public wellbeing
Raising system maturity

Figure2. Service blueprint

Figure3. System thinking mapping
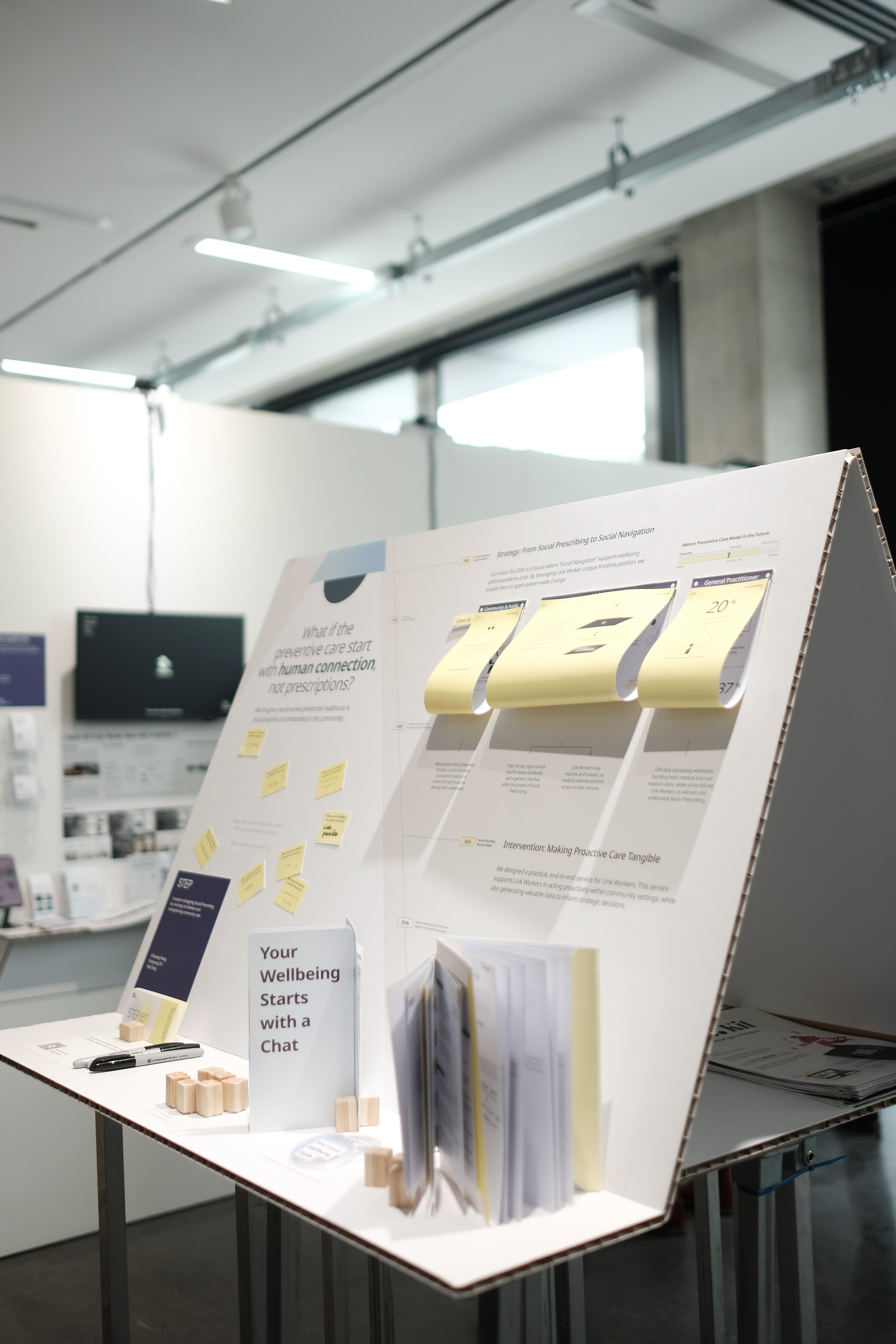
#Reactive in 2025 and Proactive Social Prescribing in the future
Social prescribing can take different forms depending on when support is offered.
>Reactive social prescribing typically begins after a problem has already appeared. It focuses on responding to needs and connecting people with community support to prevent things from getting worse. While still preventative, it works more as a safety net.
>Proactive social prescribing focuses on reaching people before problems take hold. It supports those who may feel fine or just slightly off balance, offering gentle encouragement to stay well for longer. It still involves connecting people with local activities and resources, but the emphasis is on everyday wellbeing, building resilience, and preventing future challenges, rather than responding to problems after they arise.
We have used the chart below to combine the patient's Health Stage with the different types and levels of SP needed to help us better understand and communicate with other stakeholders during the meeting. (Figure4. User stage map) Today’s system is reactive, it typically comes into play after pre-crisis health stage. However, we believe SP has the potential not only to address social issues but also to help individuals maintain their health and enhance overall wellbeing. In this way, SP could shift towards being used primarily as a proactive model.

Figure4. User stage map
#Problem statement
SP struggles to show meaningful preventive outcomes, due to systemic dependence on medical channels and the operational disempowerment of Link Workers.


Figure5. Theory of change

Figure6. MLP framework


Figure7. Link Worker role development


Figure 8. Future Roadmap with 3 Horizons
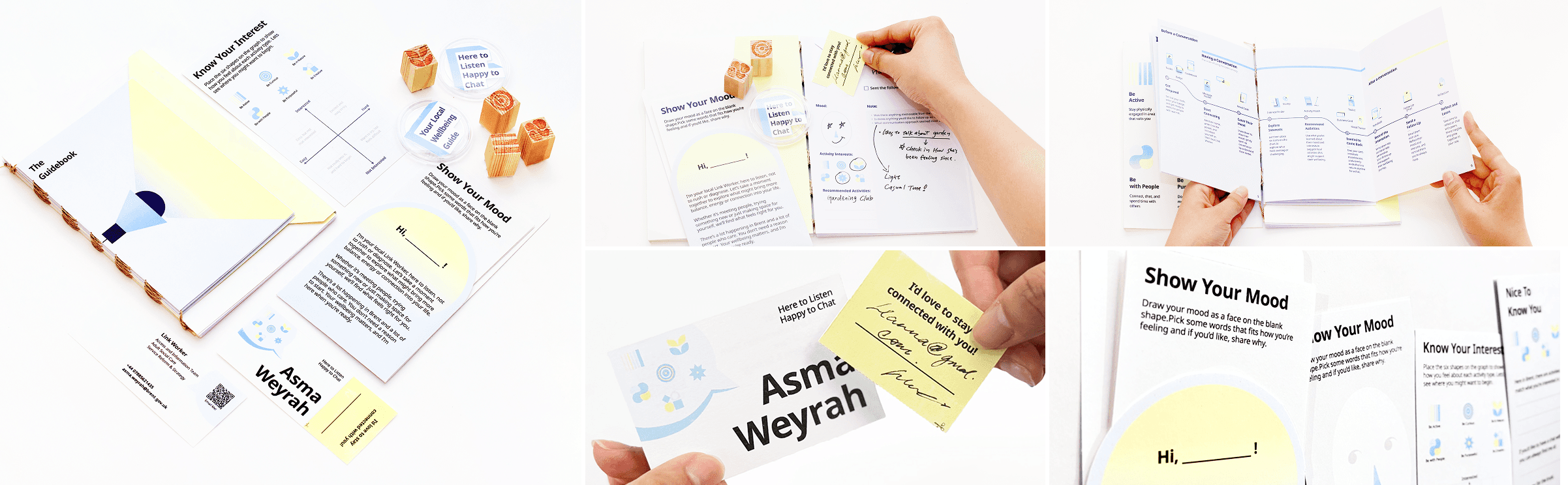

Figure10. Toolkits usage flow
The included guide¬ebook introduce the concept of proactive Social Prescribing and explain the evolving role of LWs within this new context. They also offer step-by-step instructions for using each toolkit element during real-world interactions.
Design-wise, we intentionally kept many "human" touchpoints. For example, our testing showed that writing the participant’s name on a visible card in the LW’s own handwriting creates a strong sense of personal connection and approachability. This aligns with research in social psychology suggesting that handwriting conveys authenticity and warmth, enhancing interpersonal trust (Mueller & Oppenheimer, 2014).
We introduced the toolkit to Link Workers at Brent Council and tested with more general public (Figure11), and feedback was overwhelmingly positive. Participants described the toolkit as friendly, creative, and engaging, one participant said it “immediately gives a feeling of getting to know each other.” LWs valued the toolkit’s practical design and appreciated how it supported proactive engagement while enabling the collection of meaningful data to demonstrate impact over time.

Figure11.1. At Brent Council with one Link Worker
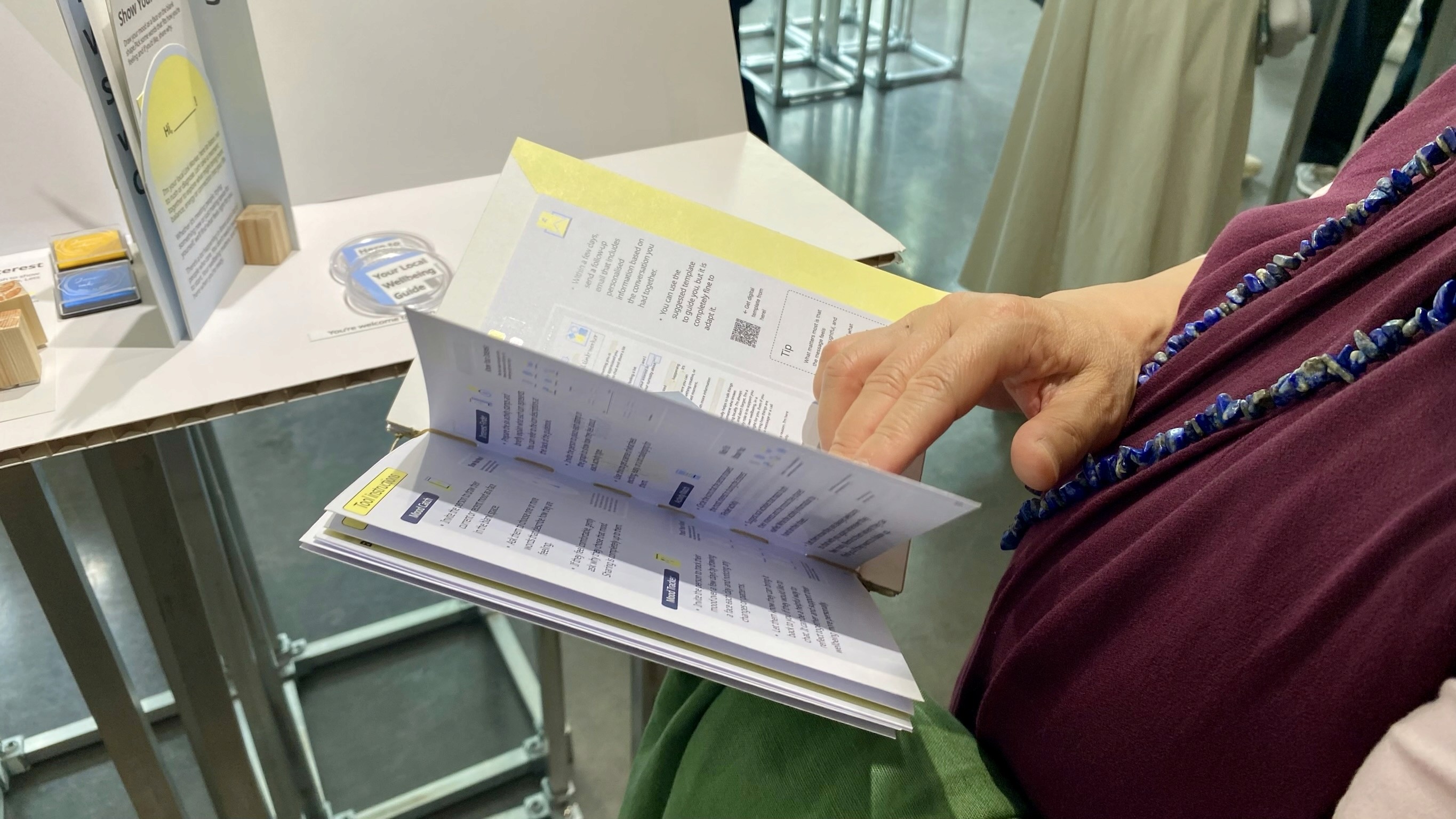
Figure11.2. Introducing toolkit to the public

Figure12. Iteration journey
We co-designed the solution closely with Link Workers, grounding our understanding of their real needs through on-the-ground research. To refine the toolkit before introducing it to actual service users, we ran a series of role-play workshops. This approach was intentional: since our future vision involves engaging healthy members of the public rather than patients, we avoided testing immature ideas directly on vulnerable groups.
Each role-play involved over 8 participants of diverse ages and genders, simulating typical interactions LWs might have in community settings. Through these sessions, we explored public responses and validated the overall flow of conversations. A key insight was that participants expressed trust in the LW and showed willingness to try recommended activities. One participant even mentioned they would be willing to become a volunteer later to support more people, highlighting the toolkit’s potential to foster genuine connections and motivate engagement.
Following these tests, we delivered the refined toolkit to Link Workers for ongoing validation and iteration in real-world contexts.
If there’s one key takeaway from this final chapter of my RCA journey, it’s that service design isn’t a magic, a "perfect" solution, it’s often a frustrating process of building trust, shifting deeply ingrained mindsets, and carving out space for new ways of working. When I first finished this project, I felt an overwhelming emptiness. The weight of social issues like health inequality and systemic barriers felt massive and complex — frankly, impossible for me, my team, or service design methods alone to fix.
But over time, through reflection, I realised the true value of service designers: we spark conversations, connect siloed actors and departments, and mix diverse ideas and disciplines to slowly change cultures and systems from within. The very challenges of our role — being outsiders, facilitators, and collaborators — become strengths, helping us narrow gaps that others can’t.
It’s about planting seeds and patiently watching them grow into fields of flowers. The people within these systems are all talented, they just need someone creates spaces for them to shine.
Ultimately, tackling social issues demands collective, persistent effort. Designers can be catalysts and facilitators, but real change requires system-wide commitment and collaboration at every level.

Thank you for your reading.
For more details about this project, see the report below!

